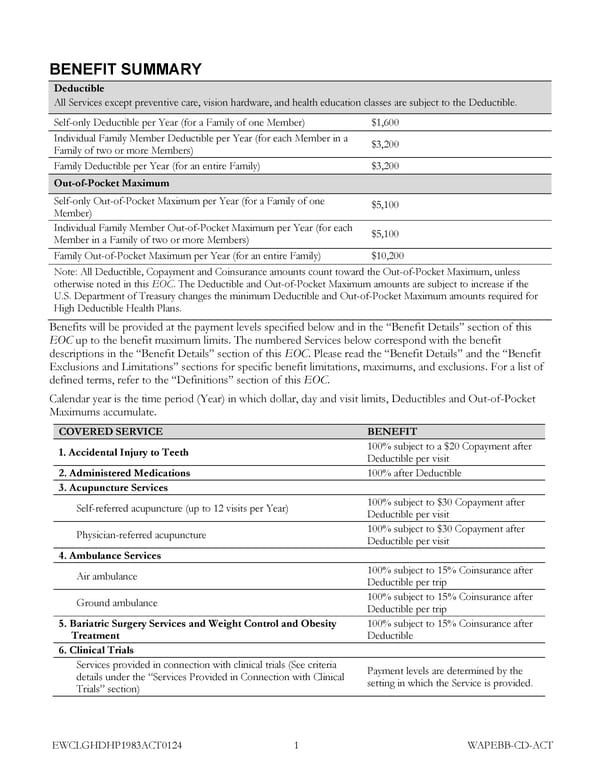
BENEFIT SUMMARY Deductible All Services except preventive care, vision hardware, and health education classes are subject to the Deductible. Self-only Deductible per Year (for a Family of one Member) $1,600 Individual Family Member Deductible per Year (for each Member in a $3,200 Family of two or more Members) Family Deductible per Year (for an entire Family) $3,200 Out-of-Pocket Maximum Self-only Out-of-Pocket Maximum per Year (for a Family of one $5,100 Member) Individual Family Member Out-of-Pocket Maximum per Year (for each $5,100 Member in a Family of two or more Members) Family Out-of-Pocket Maximum per Year (for an entire Family) $10,200 Note: All Deductible, Copayment and Coinsurance amounts count toward the Out-of-Pocket Maximum, unless otherwise noted in this EOC. The Deductible and Out-of-Pocket Maximum amounts are subject to increase if the U.S. Department of Treasury changes the minimum Deductible and Out-of-Pocket Maximum amounts required for High Deductible Health Plans. Benefits will be provided at the payment levels specified below and in the “Benefit Details” section of this EOC up to the benefit maximum limits. The numbered Services below correspond with the benefit descriptions in the “Benefit Details” section of this EOC. Please read the “Benefit Details” and the “Benefit Exclusions and Limitations” sections for specific benefit limitations, maximums, and exclusions. For a list of defined terms, refer to the “Definitions” section of this EOC. Calendar year is the time period (Year) in which dollar, day and visit limits, Deductibles and Out-of-Pocket Maximums accumulate. COVERED SERVICE BENEFIT 1. Accidental Injury to Teeth 100% subject to a $20 Copayment after Deductible per visit 2. Administered Medications 100% after Deductible 3. Acupuncture Services Self-referred acupuncture (up to 12 visits per Year) 100% subject to $30 Copayment after Deductible per visit Physician-referred acupuncture 100% subject to $30 Copayment after Deductible per visit 4. Ambulance Services Air ambulance 100% subject to 15% Coinsurance after Deductible per trip Ground ambulance 100% subject to 15% Coinsurance after Deductible per trip 5. Bariatric Surgery Services and Weight Control and Obesity 100% subject to 15% Coinsurance after Treatment Deductible 6. Clinical Trials Services provided in connection with clinical trials (See criteria Payment levels are determined by the details under the “Services Provided in Connection with Clinical setting in which the Service is provided. Trials” section) EWCLGHDHP1983ACT0124 1 WAPEBB-CD-ACT
 Kaiser Permanente NW CDHP EOC (2024) Page 7 Page 9
Kaiser Permanente NW CDHP EOC (2024) Page 7 Page 9