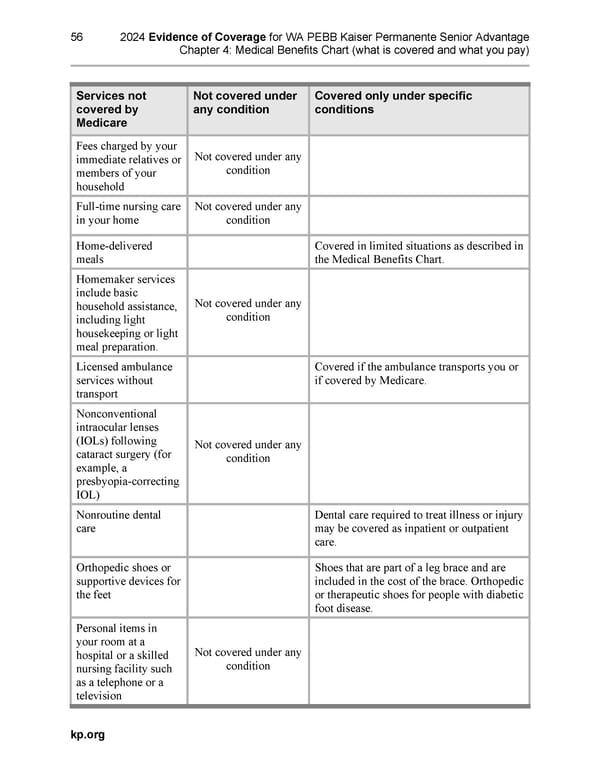
56 2024 Evidence of Coverage for WA PEBB Kaiser Permanente Senior Advantage Chapter 4: Medical Benefits Chart (what is covered and what you pay) Services not Not covered under Covered only under specific covered by any condition conditions Medicare Fees charged by your Not covered under any immediate relatives or condition members of your household Full-time nursing care Not covered under any in your home condition Home-delivered Covered in limited situations as described in meals the Medical Benefits Chart. Homemaker services include basic Not covered under any household assistance, condition including light housekeeping or light meal preparation. Licensed ambulance Covered if the ambulance transports you or services without if covered by Medicare. transport Nonconventional intraocular lenses (IOLs) following Not covered under any cataract surgery (for condition example, a presbyopia-correcting IOL) Nonroutine dental Dental care required to treat illness or injury care may be covered as inpatient or outpatient care. Orthopedic shoes or Shoes that are part of a leg brace and are supportive devices for included in the cost of the brace. Orthopedic the feet or therapeutic shoes for people with diabetic foot disease. Personal items in your room at a Not covered under any hospital or a skilled condition nursing facility such as a telephone or a television kp.org
 Kaiser Permanente NW Senior Advantage EOC (2024) Page 93 Page 95
Kaiser Permanente NW Senior Advantage EOC (2024) Page 93 Page 95