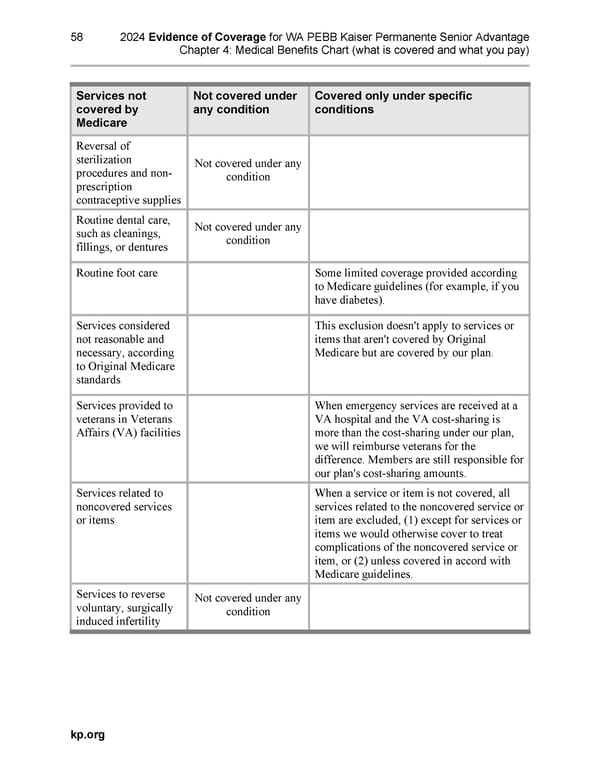
58 2024 Evidence of Coverage for WA PEBB Kaiser Permanente Senior Advantage Chapter 4: Medical Benefits Chart (what is covered and what you pay) Services not Not covered under Covered only under specific covered by any condition conditions Medicare Reversal of sterilization Not covered under any procedures and non- condition prescription contraceptive supplies Routine dental care, Not covered under any such as cleanings, condition fillings, or dentures Routine foot care Some limited coverage provided according to Medicare guidelines (for example, if you have diabetes). Services considered This exclusion doesn't apply to services or not reasonable and items that aren't covered by Original necessary, according Medicare but are covered by our plan. to Original Medicare standards Services provided to When emergency services are received at a veterans in Veterans VA hospital and the VA cost-sharing is Affairs (VA) facilities more than the cost-sharing under our plan, we will reimburse veterans for the difference. Members are still responsible for our plan's cost-sharing amounts. Services related to When a service or item is not covered, all noncovered services services related to the noncovered service or or items item are excluded, (1) except for services or items we would otherwise cover to treat complications of the noncovered service or item, or (2) unless covered in accord with Medicare guidelines. Services to reverse Not covered under any voluntary, surgically condition induced infertility kp.org
 Kaiser Permanente NW Senior Advantage EOC (2024) Page 95 Page 97
Kaiser Permanente NW Senior Advantage EOC (2024) Page 95 Page 97