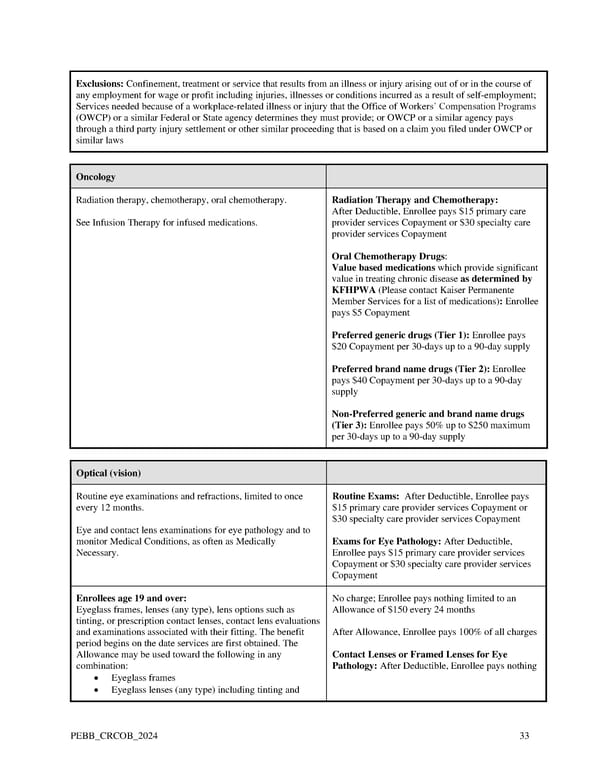
Exclusions: Confinement, treatment or service that results from an illness or injury arising out of or in the course of any employment for wage or profit including injuries, illnesses or conditions incurred as a result of self-employment; Services needed because of a workplace-related illness or injury that the Office of Workers’ Compensation Programs (OWCP) or a similar Federal or State agency determines they must provide; or OWCP or a similar agency pays through a third party injury settlement or other similar proceeding that is based on a claim you filed under OWCP or similar laws Oncology Radiation therapy, chemotherapy, oral chemotherapy. Radiation Therapy and Chemotherapy: After Deductible, Enrollee pays $15 primary care See Infusion Therapy for infused medications. provider services Copayment or $30 specialty care provider services Copayment Oral Chemotherapy Drugs: Value based medications which provide significant value in treating chronic disease as determined by KFHPWA (Please contact Kaiser Permanente Member Services for a list of medications): Enrollee pays $5 Copayment Preferred generic drugs (Tier 1): Enrollee pays $20 Copayment per 30-days up to a 90-day supply Preferred brand name drugs (Tier 2): Enrollee pays $40 Copayment per 30-days up to a 90-day supply Non-Preferred generic and brand name drugs (Tier 3): Enrollee pays 50% up to $250 maximum per 30-days up to a 90-day supply Optical (vision) Routine eye examinations and refractions, limited to once Routine Exams: After Deductible, Enrollee pays every 12 months. $15 primary care provider services Copayment or $30 specialty care provider services Copayment Eye and contact lens examinations for eye pathology and to monitor Medical Conditions, as often as Medically Exams for Eye Pathology: After Deductible, Necessary. Enrollee pays $15 primary care provider services Copayment or $30 specialty care provider services Copayment Enrollees age 19 and over: No charge; Enrollee pays nothing limited to an Eyeglass frames, lenses (any type), lens options such as Allowance of $150 every 24 months tinting, or prescription contact lenses, contact lens evaluations and examinations associated with their fitting. The benefit After Allowance, Enrollee pays 100% of all charges period begins on the date services are first obtained. The Allowance may be used toward the following in any Contact Lenses or Framed Lenses for Eye combination: Pathology: After Deductible, Enrollee pays nothing • Eyeglass frames • Eyeglass lenses (any type) including tinting and PEBB_CRCOB_2024 33
 Kaiser Permanente WA Original Medicare EOC (2024) Page 32 Page 34
Kaiser Permanente WA Original Medicare EOC (2024) Page 32 Page 34