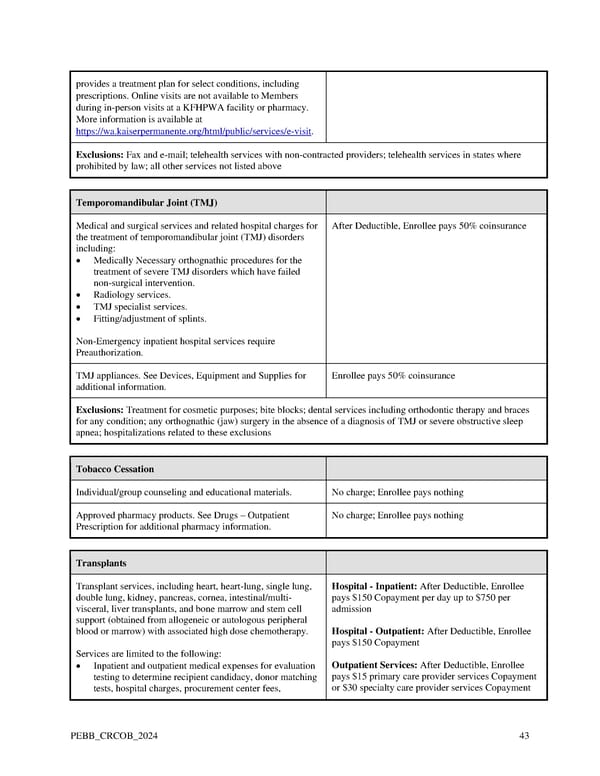
provides a treatment plan for select conditions, including prescriptions. Online visits are not available to Members during in-person visits at a KFHPWA facility or pharmacy. More information is available at https://wa.kaiserpermanente.org/html/public/services/e-visit. Exclusions: Fax and e-mail; telehealth services with non-contracted providers; telehealth services in states where prohibited by law; all other services not listed above Temporomandibular Joint (TMJ) Medical and surgical services and related hospital charges for After Deductible, Enrollee pays 50% coinsurance the treatment of temporomandibular joint (TMJ) disorders including: • Medically Necessary orthognathic procedures for the treatment of severe TMJ disorders which have failed non-surgical intervention. • Radiology services. • TMJ specialist services. • Fitting/adjustment of splints. Non-Emergency inpatient hospital services require Preauthorization. TMJ appliances. See Devices, Equipment and Supplies for Enrollee pays 50% coinsurance additional information. Exclusions: Treatment for cosmetic purposes; bite blocks; dental services including orthodontic therapy and braces for any condition; any orthognathic (jaw) surgery in the absence of a diagnosis of TMJ or severe obstructive sleep apnea; hospitalizations related to these exclusions Tobacco Cessation Individual/group counseling and educational materials. No charge; Enrollee pays nothing Approved pharmacy products. See Drugs – Outpatient No charge; Enrollee pays nothing Prescription for additional pharmacy information. Transplants Transplant services, including heart, heart-lung, single lung, Hospital - Inpatient: After Deductible, Enrollee double lung, kidney, pancreas, cornea, intestinal/multi- pays $150 Copayment per day up to $750 per visceral, liver transplants, and bone marrow and stem cell admission support (obtained from allogeneic or autologous peripheral blood or marrow) with associated high dose chemotherapy. Hospital - Outpatient: After Deductible, Enrollee pays $150 Copayment Services are limited to the following: • Inpatient and outpatient medical expenses for evaluation Outpatient Services: After Deductible, Enrollee testing to determine recipient candidacy, donor matching pays $15 primary care provider services Copayment tests, hospital charges, procurement center fees, or $30 specialty care provider services Copayment PEBB_CRCOB_2024 43
 Kaiser Permanente WA Original Medicare EOC (2024) Page 42 Page 44
Kaiser Permanente WA Original Medicare EOC (2024) Page 42 Page 44