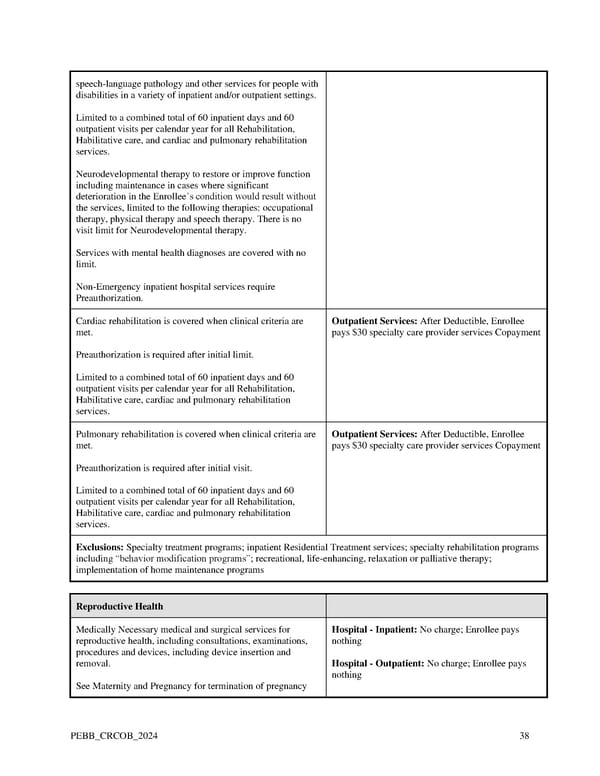
speech-language pathology and other services for people with disabilities in a variety of inpatient and/or outpatient settings. Limited to a combined total of 60 inpatient days and 60 outpatient visits per calendar year for all Rehabilitation, Habilitative care, and cardiac and pulmonary rehabilitation services. Neurodevelopmental therapy to restore or improve function including maintenance in cases where significant deterioration in the Enrollee’s condition would result without the services, limited to the following therapies: occupational therapy, physical therapy and speech therapy. There is no visit limit for Neurodevelopmental therapy. Services with mental health diagnoses are covered with no limit. Non-Emergency inpatient hospital services require Preauthorization. Cardiac rehabilitation is covered when clinical criteria are Outpatient Services: After Deductible, Enrollee met. pays $30 specialty care provider services Copayment Preauthorization is required after initial limit. Limited to a combined total of 60 inpatient days and 60 outpatient visits per calendar year for all Rehabilitation, Habilitative care, cardiac and pulmonary rehabilitation services. Pulmonary rehabilitation is covered when clinical criteria are Outpatient Services: After Deductible, Enrollee met. pays $30 specialty care provider services Copayment Preauthorization is required after initial visit. Limited to a combined total of 60 inpatient days and 60 outpatient visits per calendar year for all Rehabilitation, Habilitative care, cardiac and pulmonary rehabilitation services. Exclusions: Specialty treatment programs; inpatient Residential Treatment services; specialty rehabilitation programs including “behavior modification programs”; recreational, life-enhancing, relaxation or palliative therapy; implementation of home maintenance programs Reproductive Health Medically Necessary medical and surgical services for Hospital - Inpatient: No charge; Enrollee pays reproductive health, including consultations, examinations, nothing procedures and devices, including device insertion and removal. Hospital - Outpatient: No charge; Enrollee pays nothing See Maternity and Pregnancy for termination of pregnancy PEBB_CRCOB_2024 38
 Kaiser Permanente WA Original Medicare EOC (2024) Page 37 Page 39
Kaiser Permanente WA Original Medicare EOC (2024) Page 37 Page 39