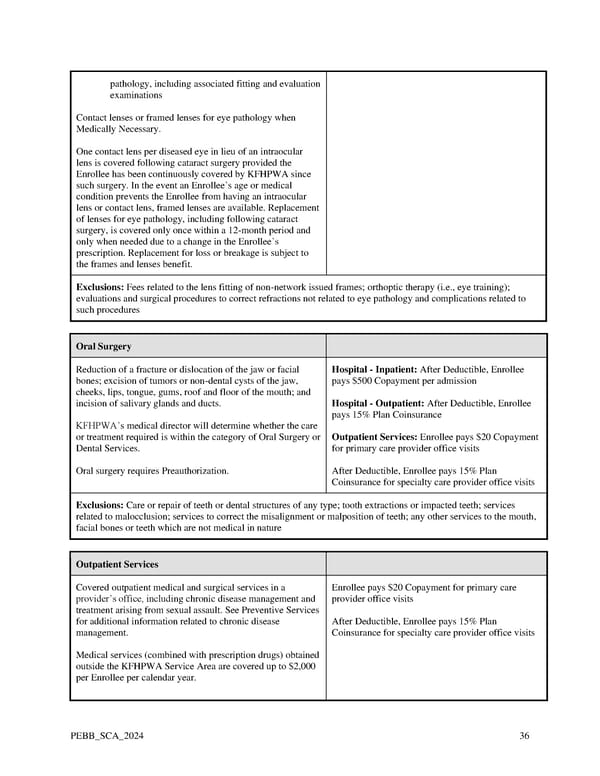
pathology, including associated fitting and evaluation examinations Contact lenses or framed lenses for eye pathology when Medically Necessary. One contact lens per diseased eye in lieu of an intraocular lens is covered following cataract surgery provided the Enrollee has been continuously covered by KFHPWA since such surgery. In the event an Enrollee’s age or medical condition prevents the Enrollee from having an intraocular lens or contact lens, framed lenses are available. Replacement of lenses for eye pathology, including following cataract surgery, is covered only once within a 12-month period and only when needed due to a change in the Enrollee’s prescription. Replacement for loss or breakage is subject to the frames and lenses benefit. Exclusions: Fees related to the lens fitting of non-network issued frames; orthoptic therapy (i.e., eye training); evaluations and surgical procedures to correct refractions not related to eye pathology and complications related to such procedures Oral Surgery Reduction of a fracture or dislocation of the jaw or facial Hospital - Inpatient: After Deductible, Enrollee bones; excision of tumors or non-dental cysts of the jaw, pays $500 Copayment per admission cheeks, lips, tongue, gums, roof and floor of the mouth; and incision of salivary glands and ducts. Hospital - Outpatient: After Deductible, Enrollee pays 15% Plan Coinsurance KFHPWA’s medical director will determine whether the care or treatment required is within the category of Oral Surgery or Outpatient Services: Enrollee pays $20 Copayment Dental Services. for primary care provider office visits Oral surgery requires Preauthorization. After Deductible, Enrollee pays 15% Plan Coinsurance for specialty care provider office visits Exclusions: Care or repair of teeth or dental structures of any type; tooth extractions or impacted teeth; services related to malocclusion; services to correct the misalignment or malposition of teeth; any other services to the mouth, facial bones or teeth which are not medical in nature Outpatient Services Covered outpatient medical and surgical services in a Enrollee pays $20 Copayment for primary care provider’s office, including chronic disease management and provider office visits treatment arising from sexual assault. See Preventive Services for additional information related to chronic disease After Deductible, Enrollee pays 15% Plan management. Coinsurance for specialty care provider office visits Medical services (combined with prescription drugs) obtained outside the KFHPWA Service Area are covered up to $2,000 per Enrollee per calendar year. PEBB_SCA_2024 36
 Kaiser Permanente WA SoundChoice EOC (2024) Page 35 Page 37
Kaiser Permanente WA SoundChoice EOC (2024) Page 35 Page 37