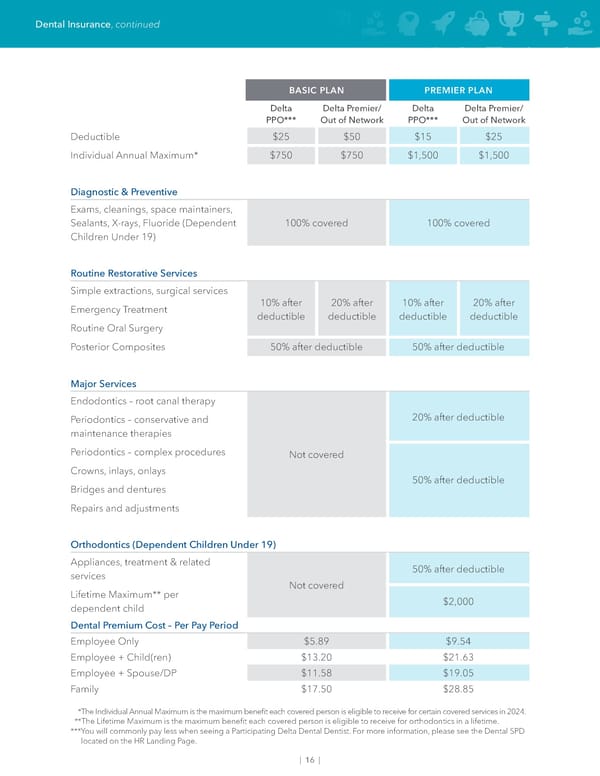
Dental Insurance, continued BASIC PLAN PREMIER PLAN Delta Delta Premier/ Delta Delta Premier/ PPO*** Out of Network PPO*** Out of Network Deductible $25 $50 $15 $25 Individual Annual Maximum* $750 $750 $1,500 $1,500 Diagnostic & Preventive Exams, cleanings, space maintainers, Sealants, X-rays, Fluoride (Dependent 100% covered 100% covered Children Under 19) Routine Restorative Services Simple extractions, surgical services Emergency Treatment 10% after 20% after 10% after 20% after deductible deductible deductible deductible Routine Oral Surgery Posterior Composites 50% after deductible 50% after deductible Major Services Endodontics – root canal therapy Periodontics – conservative and 20% after deductible maintenance therapies Periodontics – complex procedures Not covered Crowns, inlays, onlays 50% after deductible Bridges and dentures Repairs and adjustments Orthodontics (Dependent Children Under 19) Appliances, treatment & related 50% after deductible services Not covered Lifetime Maximum** per $2,000 dependent child Dental Premium Cost – Per Pay Period Employee Only $5.89 $9.54 Employee + Child(ren) $13.20 $21.63 Employee + Spouse/DP $11.58 $19.05 Family $17.50 $28.85 *The Individual Annual Maximum is the maximum bene昀椀t each covered person is eligible to receive for certain covered services in 2024. **The Lifetime Maximum is the maximum bene昀椀t each covered person is eligible to receive for orthodontics in a lifetime. *** You will commonly pay less when seeing a Participating Delta Dental Dentist. For more information, please see the Dental SPD located on the HR Landing Page. | 16 |
 May 2024 | Dubuque Union Team Members Benefit Guide Page 17 Page 19
May 2024 | Dubuque Union Team Members Benefit Guide Page 17 Page 19