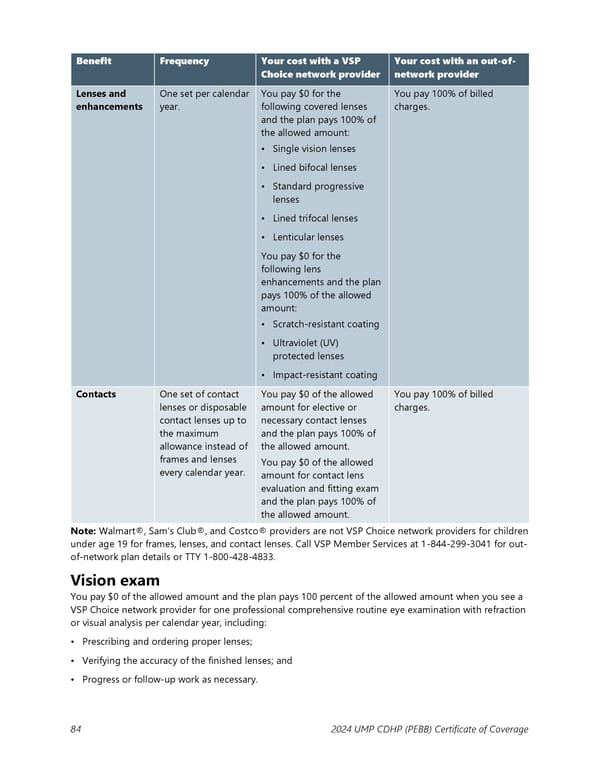
Benefit Frequency Your cost with a VSP Your cost with an out-of- Choice network provider network provider Lenses and One set per calendar You pay $0 for the You pay 100% of billed enhancements year. following covered lenses charges. and the plan pays 100% of the allowed amount: • Single vision lenses • Lined bifocal lenses • Standard progressive lenses • Lined trifocal lenses • Lenticular lenses You pay $0 for the following lens enhancements and the plan pays 100% of the allowed amount: • Scratch-resistant coating • Ultraviolet (UV) protected lenses • Impact-resistant coating Contacts One set of contact You pay $0 of the allowed You pay 100% of billed lenses or disposable amount for elective or charges. contact lenses up to necessary contact lenses the maximum and the plan pays 100% of allowance instead of the allowed amount. frames and lenses You pay $0 of the allowed every calendar year. amount for contact lens evaluation and fitting exam and the plan pays 100% of the allowed amount. Note: Walmart®, Sam’s Club®, and Costco® providers are not VSP Choice network providers for children under age 19 for frames, lenses, and contact lenses. Call VSP Member Services at 1-844-299-3041 for out- of-network plan details or TTY 1-800-428-4833. Vision exam You pay $0 of the allowed amount and the plan pays 100 percent of the allowed amount when you see a VSP Choice network provider for one professional comprehensive routine eye examination with refraction or visual analysis per calendar year, including: • Prescribing and ordering proper lenses; • Verifying the accuracy of the finished lenses; and • Progress or follow-up work as necessary. 84 2024 UMP CDHP (PEBB) Certificate of Coverage
 UMP Consumer-Directed Health Plan (CDHP) COC (2024) Page 84 Page 86
UMP Consumer-Directed Health Plan (CDHP) COC (2024) Page 84 Page 86