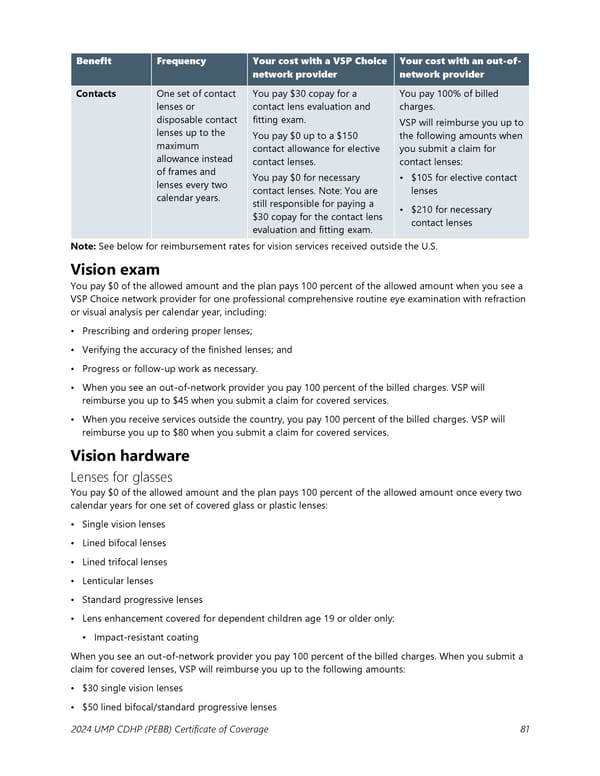
Benefit Frequency Your cost with a VSP Choice Your cost with an out-of- network provider network provider Contacts One set of contact You pay $30 copay for a You pay 100% of billed lenses or contact lens evaluation and charges. disposable contact fitting exam. VSP will reimburse you up to lenses up to the You pay $0 up to a $150 the following amounts when maximum contact allowance for elective you submit a claim for allowance instead contact lenses. contact lenses: of frames and You pay $0 for necessary • $105 for elective contact lenses every two contact lenses. Note: You are lenses calendar years. still responsible for paying a • $210 for necessary $30 copay for the contact lens contact lenses evaluation and fitting exam. Note: See below for reimbursement rates for vision services received outside the U.S. Vision exam You pay $0 of the allowed amount and the plan pays 100 percent of the allowed amount when you see a VSP Choice network provider for one professional comprehensive routine eye examination with refraction or visual analysis per calendar year, including: • Prescribing and ordering proper lenses; • Verifying the accuracy of the finished lenses; and • Progress or follow-up work as necessary. • When you see an out-of-network provider you pay 100 percent of the billed charges. VSP will reimburse you up to $45 when you submit a claim for covered services. • When you receive services outside the country, you pay 100 percent of the billed charges. VSP will reimburse you up to $80 when you submit a claim for covered services. Vision hardware Lenses for glasses You pay $0 of the allowed amount and the plan pays 100 percent of the allowed amount once every two calendar years for one set of covered glass or plastic lenses: • Single vision lenses • Lined bifocal lenses • Lined trifocal lenses • Lenticular lenses • Standard progressive lenses • Lens enhancement covered for dependent children age 19 or older only: ▪ Impact-resistant coating When you see an out-of-network provider you pay 100 percent of the billed charges. When you submit a claim for covered lenses, VSP will reimburse you up to the following amounts: • $30 single vision lenses • $50 lined bifocal/standard progressive lenses 2024 UMP CDHP (PEBB) Certificate of Coverage 81
 UMP Consumer-Directed Health Plan (CDHP) COC (2024) Page 81 Page 83
UMP Consumer-Directed Health Plan (CDHP) COC (2024) Page 81 Page 83