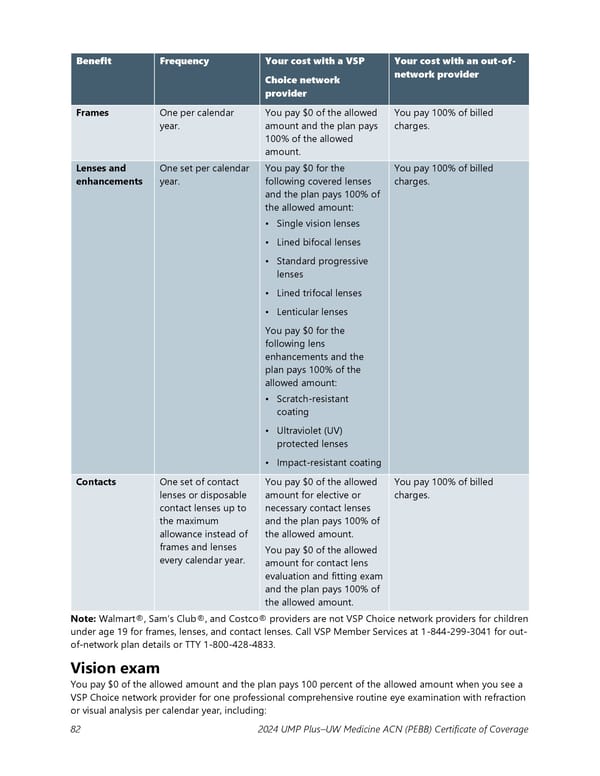
Benefit Frequency Your cost with a VSP Your cost with an out-of- Choice network network provider provider Frames One per calendar You pay $0 of the allowed You pay 100% of billed year. amount and the plan pays charges. 100% of the allowed amount. Lenses and One set per calendar You pay $0 for the You pay 100% of billed enhancements year. following covered lenses charges. and the plan pays 100% of the allowed amount: • Single vision lenses • Lined bifocal lenses • Standard progressive lenses • Lined trifocal lenses • Lenticular lenses You pay $0 for the following lens enhancements and the plan pays 100% of the allowed amount: • Scratch-resistant coating • Ultraviolet (UV) protected lenses • Impact-resistant coating Contacts One set of contact You pay $0 of the allowed You pay 100% of billed lenses or disposable amount for elective or charges. contact lenses up to necessary contact lenses the maximum and the plan pays 100% of allowance instead of the allowed amount. frames and lenses You pay $0 of the allowed every calendar year. amount for contact lens evaluation and fitting exam and the plan pays 100% of the allowed amount. Note: Walmart®, Sam’s Club®, and Costco® providers are not VSP Choice network providers for children under age 19 for frames, lenses, and contact lenses. Call VSP Member Services at 1-844-299-3041 for out- of-network plan details or TTY 1-800-428-4833. Vision exam You pay $0 of the allowed amount and the plan pays 100 percent of the allowed amount when you see a VSP Choice network provider for one professional comprehensive routine eye examination with refraction or visual analysis per calendar year, including: 82 2024 UMP Plus–UW Medicine ACN (PEBB) Certificate of Coverage
 UMP Plus–UW Medicine Accountable Care Network (UW Medicine ACN) COC (2024) Page 82 Page 84
UMP Plus–UW Medicine Accountable Care Network (UW Medicine ACN) COC (2024) Page 82 Page 84