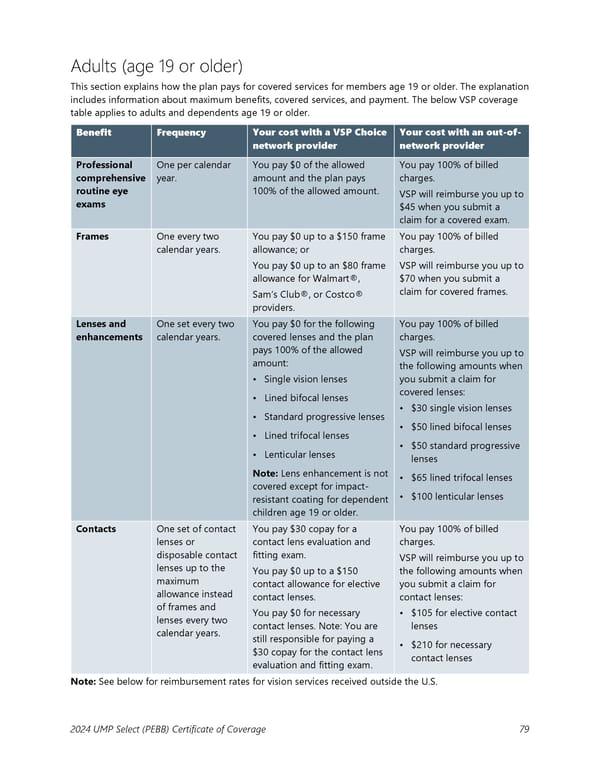
Adults (age 19 or older) This section explains how the plan pays for covered services for members age 19 or older. The explanation includes information about maximum benefits, covered services, and payment. The below VSP coverage table applies to adults and dependents age 19 or older. Benefit Frequency Your cost with a VSP Choice Your cost with an out-of- network provider network provider Professional One per calendar You pay $0 of the allowed You pay 100% of billed comprehensive year. amount and the plan pays charges. routine eye 100% of the allowed amount. VSP will reimburse you up to exams $45 when you submit a claim for a covered exam. Frames One every two You pay $0 up to a $150 frame You pay 100% of billed calendar years. allowance; or charges. You pay $0 up to an $80 frame VSP will reimburse you up to allowance for Walmart®, $70 when you submit a claim for covered frames. Sam’s Club®, or Costco® providers. Lenses and One set every two You pay $0 for the following You pay 100% of billed enhancements calendar years. covered lenses and the plan charges. pays 100% of the allowed VSP will reimburse you up to amount: the following amounts when • Single vision lenses you submit a claim for • Lined bifocal lenses covered lenses: • Standard progressive lenses • $30 single vision lenses • Lined trifocal lenses • $50 lined bifocal lenses • Lenticular lenses • $50 standard progressive lenses Note: Lens enhancement is not • $65 lined trifocal lenses covered except for impact- • $100 lenticular lenses resistant coating for dependent children age 19 or older. Contacts One set of contact You pay $30 copay for a You pay 100% of billed lenses or contact lens evaluation and charges. disposable contact fitting exam. VSP will reimburse you up to lenses up to the You pay $0 up to a $150 the following amounts when maximum contact allowance for elective you submit a claim for allowance instead contact lenses. contact lenses: of frames and You pay $0 for necessary • $105 for elective contact lenses every two contact lenses. Note: You are lenses calendar years. still responsible for paying a • $210 for necessary $30 copay for the contact lens contact lenses evaluation and fitting exam. Note: See below for reimbursement rates for vision services received outside the U.S. 2024 UMP Select (PEBB) Certificate of Coverage 79
 UMP Select COC (2024) Page 79 Page 81
UMP Select COC (2024) Page 79 Page 81