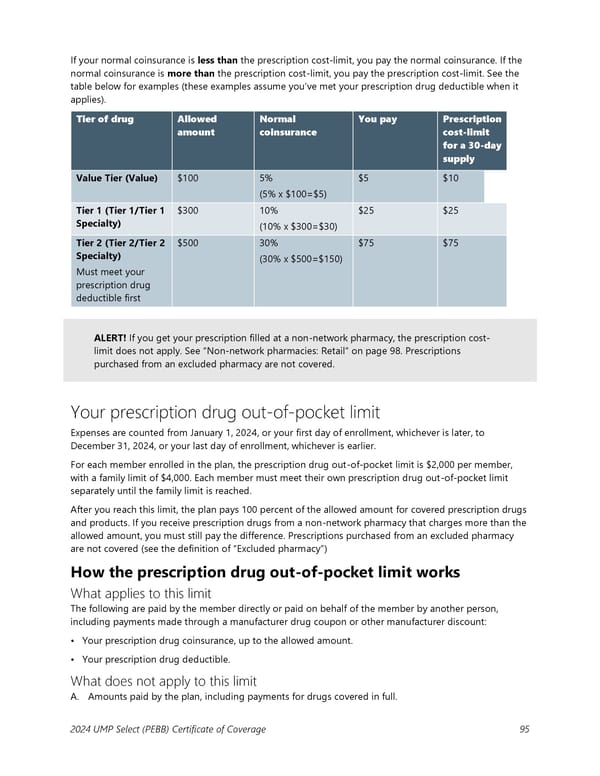
If your normal coinsurance is less than the prescription cost-limit, you pay the normal coinsurance. If the normal coinsurance is more than the prescription cost-limit, you pay the prescription cost-limit. See the table below for examples (these examples assume you’ve met your prescription drug deductible when it applies). Tier of drug Allowed Normal You pay Prescription amount coinsurance cost-limit for a 30-day supply Value Tier (Value) $100 5% $5 $10 (5% x $100=$5) Tier 1 (Tier 1/Tier 1 $300 10% $25 $25 Specialty) (10% x $300=$30) Tier 2 (Tier 2/Tier 2 $500 30% $75 $75 Specialty) (30% x $500=$150) Must meet your prescription drug deductible first ALERT! If you get your prescription filled at a non-network pharmacy, the prescription cost- limit does not apply. See “Non-network pharmacies: Retail” on page 98. Prescriptions purchased from an excluded pharmacy are not covered. Your prescription drug out-of-pocket limit Expenses are counted from January 1, 2024, or your first day of enrollment, whichever is later, to December 31, 2024, or your last day of enrollment, whichever is earlier. For each member enrolled in the plan, the prescription drug out-of-pocket limit is $2,000 per member, with a family limit of $4,000. Each member must meet their own prescription drug out-of-pocket limit separately until the family limit is reached. After you reach this limit, the plan pays 100 percent of the allowed amount for covered prescription drugs and products. If you receive prescription drugs from a non-network pharmacy that charges more than the allowed amount, you must still pay the difference. Prescriptions purchased from an excluded pharmacy are not covered (see the definition of “Excluded pharmacy”) How the prescription drug out-of-pocket limit works What applies to this limit The following are paid by the member directly or paid on behalf of the member by another person, including payments made through a manufacturer drug coupon or other manufacturer discount: • Your prescription drug coinsurance, up to the allowed amount. • Your prescription drug deductible. What does not apply to this limit A. Amounts paid by the plan, including payments for drugs covered in full. 2024 UMP Select (PEBB) Certificate of Coverage 95
 UMP Select COC (2024) Page 95 Page 97
UMP Select COC (2024) Page 95 Page 97