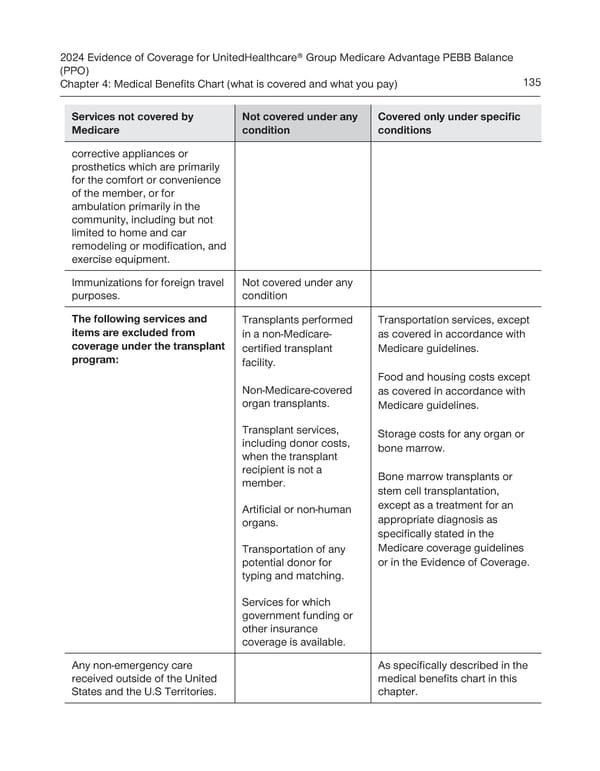
2024 Evidence of Coverage for UnitedHealthcare® Group Medicare Advantage PEBB Balance (PPO) Chapter 4: Medical Benefits Chart (what is covered and what you pay) 135 Services not covered by Not covered under any Covered only under specific Medicare condition conditions corrective appliances or prosthetics which are primarily for the comfort or convenience of the member, or for ambulation primarily in the community, including but not limited to home and car remodeling or modification, and exercise equipment. Immunizations for foreign travel Not covered under any purposes. condition The following services and Transplants performed Transportation services, except items are excluded from in a non-Medicare- as covered in accordance with coverage under the transplant certified transplant Medicare guidelines. program: facility. Food and housing costs except Non-Medicare-covered as covered in accordance with organ transplants. Medicare guidelines. Transplant services, Storage costs for any organ or including donor costs, bone marrow. when the transplant recipient is not a Bone marrow transplants or member. stem cell transplantation, Artificial or non-human except as a treatment for an organs. appropriate diagnosis as specifically stated in the Transportation of any Medicare coverage guidelines potential donor for or in the Evidence of Coverage. typing and matching. Services for which government funding or other insurance coverage is available. Any non-emergency care As specifically described in the received outside of the United medical benefits chart in this States and the U.S Territories. chapter.
 UnitedHealthcare PEBB Balance EOC (2024) Page 140 Page 142
UnitedHealthcare PEBB Balance EOC (2024) Page 140 Page 142