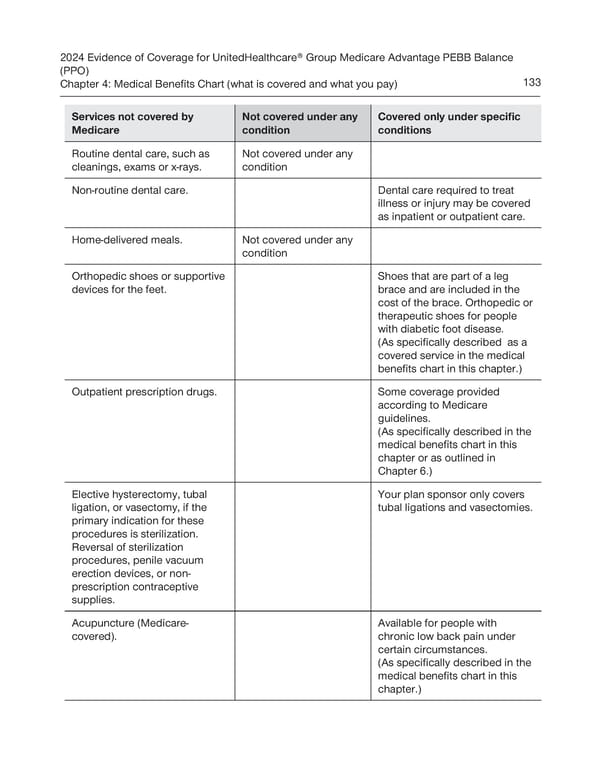
2024 Evidence of Coverage for UnitedHealthcare® Group Medicare Advantage PEBB Balance (PPO) Chapter 4: Medical Benefits Chart (what is covered and what you pay) 133 Services not covered by Not covered under any Covered only under specific Medicare condition conditions Routine dental care, such as Not covered under any cleanings, exams or x-rays. condition Non-routine dental care. Dental care required to treat illness or injury may be covered as inpatient or outpatient care. Home-delivered meals. Not covered under any condition Orthopedic shoes or supportive Shoes that are part of a leg devices for the feet. brace and are included in the cost of the brace. Orthopedic or therapeutic shoes for people with diabetic foot disease. (As specifically described as a covered service in the medical benefits chart in this chapter.) Outpatient prescription drugs. Some coverage provided according to Medicare guidelines. (As specifically described in the medical benefits chart in this chapter or as outlined in Chapter 6.) Elective hysterectomy, tubal Your plan sponsor only covers ligation, or vasectomy, if the tubal ligations and vasectomies. primary indication for these procedures is sterilization. Reversal of sterilization procedures, penile vacuum erection devices, or non- prescription contraceptive supplies. Acupuncture (Medicare- Available for people with covered). chronic low back pain under certain circumstances. (As specifically described in the medical benefits chart in this chapter.)
 UnitedHealthcare PEBB Balance EOC (2024) Page 138 Page 140
UnitedHealthcare PEBB Balance EOC (2024) Page 138 Page 140