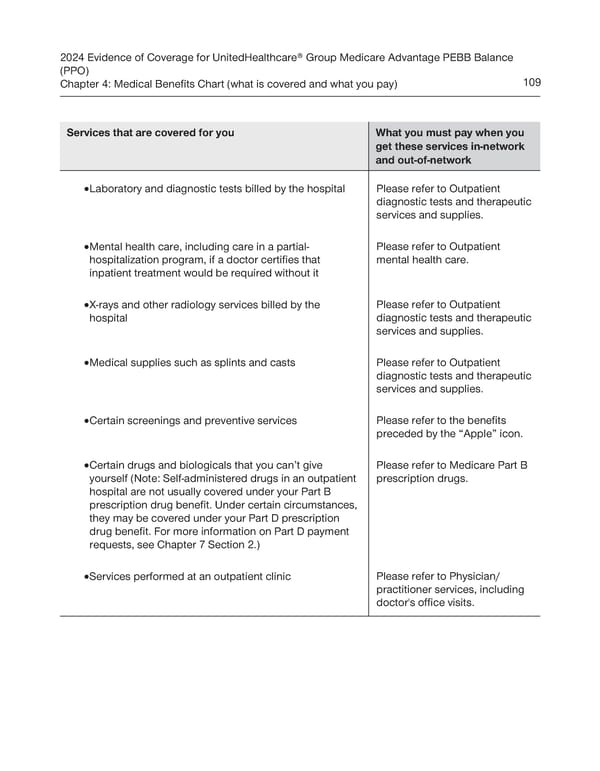
2024 Evidence of Coverage for UnitedHealthcare® Group Medicare Advantage PEBB Balance (PPO) Chapter 4: Medical Benefits Chart (what is covered and what you pay) 109 Services that are covered for you What you must pay when you get these services in-network and out-of-network · Laboratory and diagnostic tests billed by the hospital Please refer to Outpatient diagnostic tests and therapeutic services and supplies. · Mental health care, including care in a partial- Please refer to Outpatient hospitalization program, if a doctor certifies that mental health care. inpatient treatment would be required without it · X-rays and other radiology services billed by the Please refer to Outpatient hospital diagnostic tests and therapeutic services and supplies. · Medical supplies such as splints and casts Please refer to Outpatient diagnostic tests and therapeutic services and supplies. · Certain screenings and preventive services Please refer to the benefits preceded by the “Apple” icon. · Certain drugs and biologicals that you can’t give Please refer to Medicare Part B yourself (Note: Self-administered drugs in an outpatient prescription drugs. hospital are not usually covered under your Part B prescription drug benefit. Under certain circumstances, they may be covered under your Part D prescription drug benefit. For more information on Part D payment requests, see Chapter 7 Section 2.) · Services performed at an outpatient clinic Please refer to Physician/ practitioner services, including doctor's office visits.
 UnitedHealthcare PEBB Balance EOC (2024) Page 114 Page 116
UnitedHealthcare PEBB Balance EOC (2024) Page 114 Page 116