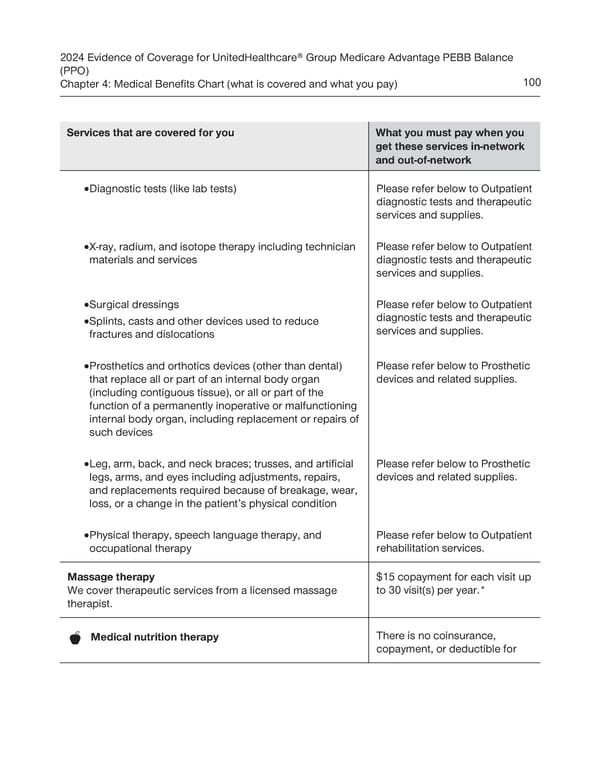
2024 Evidence of Coverage for UnitedHealthcare® Group Medicare Advantage PEBB Balance (PPO) Chapter 4: Medical Benefits Chart (what is covered and what you pay) 100 Services that are covered for you What you must pay when you get these services in-network and out-of-network · Diagnostic tests (like lab tests) Please refer below to Outpatient diagnostic tests and therapeutic services and supplies. · X-ray, radium, and isotope therapy including technician Please refer below to Outpatient materials and services diagnostic tests and therapeutic services and supplies. · Surgical dressings Please refer below to Outpatient · Splints, casts and other devices used to reduce diagnostic tests and therapeutic fractures and dislocations services and supplies. · Prosthetics and orthotics devices (other than dental) Please refer below to Prosthetic that replace all or part of an internal body organ devices and related supplies. (including contiguous tissue), or all or part of the function of a permanently inoperative or malfunctioning internal body organ, including replacement or repairs of such devices · Leg, arm, back, and neck braces; trusses, and artificial Please refer below to Prosthetic legs, arms, and eyes including adjustments, repairs, devices and related supplies. and replacements required because of breakage, wear, loss, or a change in the patient’s physical condition · Physical therapy, speech language therapy, and Please refer below to Outpatient occupational therapy rehabilitation services. Massage therapy $15 copayment for each visit up We cover therapeutic services from a licensed massage to 30 visit(s) per year.* therapist. There is no coinsurance, Medical nutrition therapy copayment, or deductible for
 UnitedHealthcare PEBB Balance EOC (2024) Page 105 Page 107
UnitedHealthcare PEBB Balance EOC (2024) Page 105 Page 107