Blue 20/20 Exam-Plus Vision Plan Overview
This document outlines the coverage details for the Blue 20/20 Exam-Plus Vision Plan, including benefits for in-network and out-of-network services, additional discounts, and frequency of covered exams and lenses.
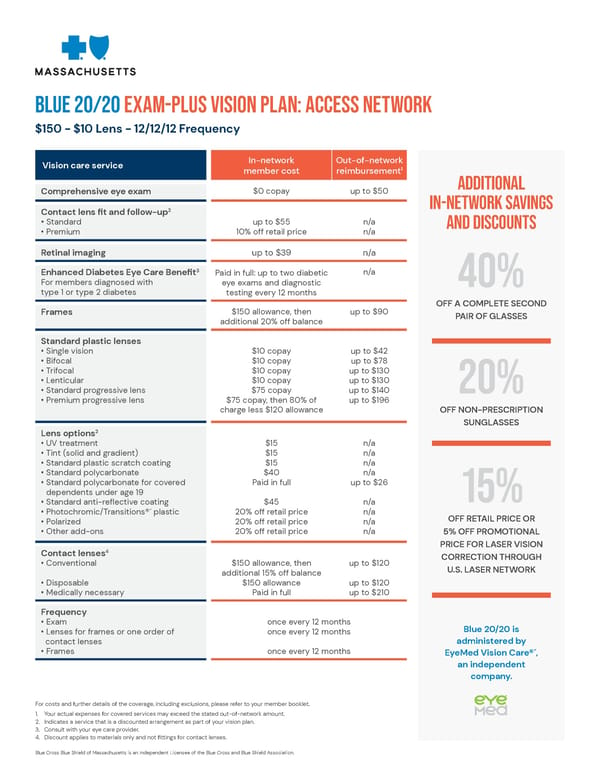
BLUE 20/20 Exam-PLUS Vision Plan: Access Network $150 - $10 Lens - 12/12/12 Frequency Vision care service In-network Out-of-network member cost reimbursement1 Comprehensive eye exam $0 copay up to $50 Additional 2 in-network savings Contact lens fit and follow-up • Standard up to $55 n/a and discounts • Premium 10% off retail price n/a Retinal imaging up to $39 n/a 3 n/a Enhanced Diabetes Eye Care Benefit Paid in full: up to two diabetic For members diagnosed with eye exams and diagnostic 40% type 1 or type 2 diabetes testing every 12 months OFF A COMPLETE SECOND Frames $150 allowance, then up to $90 PAIR OF GLASSES additional 20% off balance Standard plastic lenses • Single vision $10 copay up to $42 • Bifocal $10 copay up to $78 • Trifocal $10 copay up to $130 • Lenticular $10 copay up to $130 • Standard progressive lens $75 copay up to $140 20% • Premium progressive lens $75 copay, then 80% of up to $196 charge less $120 allowance OFF NON-PRESCRIPTION SUNGLASSES 2 Lens options • UV treatment $15 n/a • Tint (solid and gradient) $15 n/a • Standard plastic scratch coating $15 n/a • Standard polycarbonate $40 n/a • Standar d polycarbonate for covered Paid in full up to $26 dependents under age 19 15% • Standard anti-reflective coating $45 n/a • Photochromic/Transitions®´ plastic 20% off retail price n/a OFF RETAIL PRICE OR • Polarized 20% off retail price n/a • Other add-ons 20% off retail price n/a 5% OFF PROMOTIONAL PRICE FOR LASER VISION 4 Contact lenses CORRECTION THROUGH • Conventional $150 allowance, then up to $120 U.S. LASER NETWORK additional 15% off balance • Disposable $150 allowance up to $120 • Medically necessary Paid in full up to $210 Frequency • Exam once every 12 months Blue 20/20 is • Lenses for frames or one order of once every 12 months contact lenses administered by • Frames once every 12 months EyeMed Vision Care®´, an independent company. For costs and further details of the coverage, including exclusions, please refer to your member booklet. 1. Your actual expenses for covered services may exceed the stated out-of-network amount. 2. Indicates a service that is a discounted arrangement as part of your vision plan. 3. Consult with your eye care provider. 4. Discount applies to materials only and not fittings for contact lenses. Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association.
 Blue 20/20 Exam-Plus Vision Plan Overview Page 2
Blue 20/20 Exam-Plus Vision Plan Overview Page 2