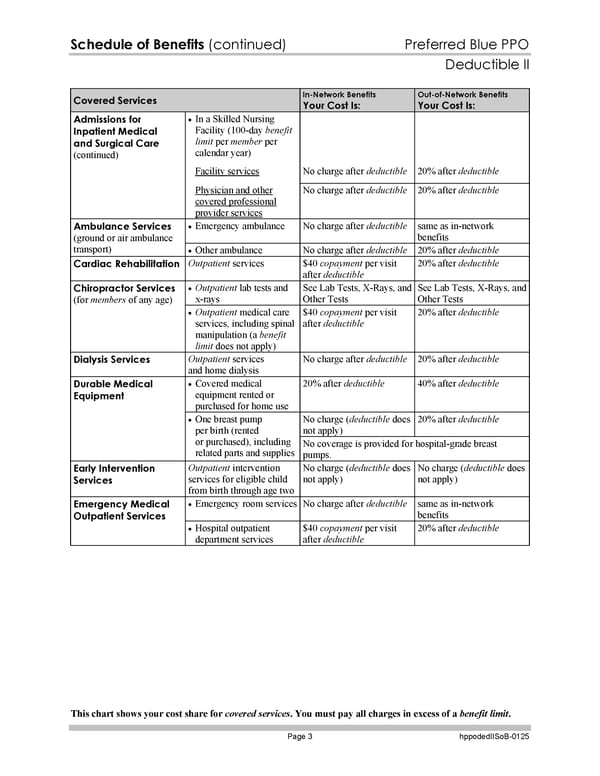
Schedule of Benefits (continued) Preferred Blue PPO Deductible II This chart shows your cost share for covered services. You must pay all charges in excess of a benefit limit. Page 3 hppodedIISoB-0125 Covered Services In-Network Benefits Your Cost Is: Out-of-Network Benefits Your Cost Is: In a Skilled Nursing Facility (100-day benefit limit per member per calendar year) Facility services No charge after deductible 20% after deductible Admissions for Inpatient Medical and Surgical Care (continued) Physician and other covered professional provider services No charge after deductible 20% after deductible Emergency ambulance No charge after deductible same as in-network benefits Ambulance Services (ground or air ambulance transport) Other ambulance No charge after deductible 20% after deductible Cardiac Rehabilitation Outpatient services $40 copayment per visit after deductible 20% after deductible Outpatient lab tests and x-rays See Lab Tests, X-Rays, and Other Tests See Lab Tests, X-Rays, and Other Tests Chiropractor Services (for members of any age) Outpatient medical care services, including spinal manipulation (a benefit limit does not apply) $40 copayment per visit after deductible 20% after deductible Dialysis Services Outpatient services and home dialysis No charge after deductible 20% after deductible Covered medical equipment rented or purchased for home use 20% after deductible 40% after deductible No charge (deductible does not apply) 20% after deductible Durable Medical Equipment One breast pump per birth (rented or purchased), including related parts and supplies No coverage is provided for hospital-grade breast pumps. Early Intervention Services Outpatient intervention services for eligible child from birth through age two No charge (deductible does not apply) No charge (deductible does not apply) Emergency room services No charge after deductible same as in-network benefits Emergency Medical Outpatient Services Hospital outpatient department services $40 copayment per visit after deductible 20% after deductible
 Blue Cross Blue Shield of Massachusetts Subscriber Information Page 129 Page 131
Blue Cross Blue Shield of Massachusetts Subscriber Information Page 129 Page 131