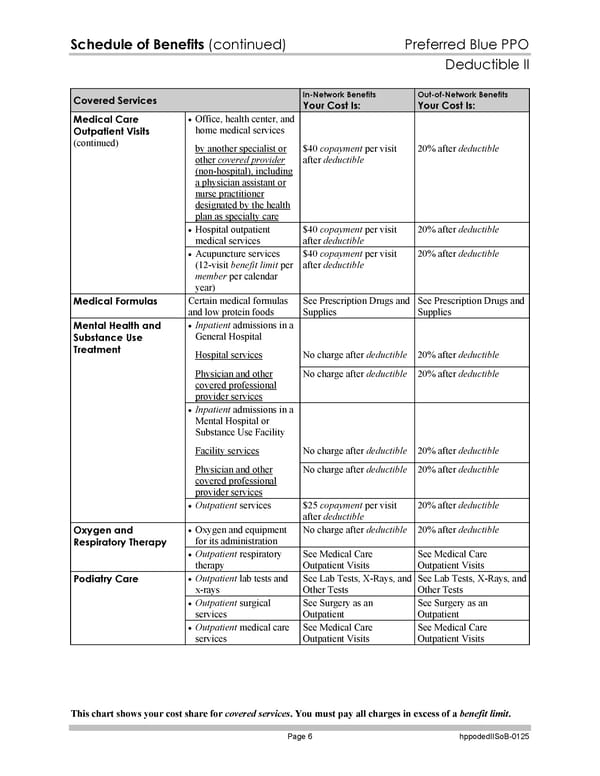
Schedule of Benefits (continued) Preferred Blue PPO Deductible II This chart shows your cost share for covered services. You must pay all charges in excess of a benefit limit. Page 6 hppodedIISoB-0125 Covered Services In-Network Benefits Your Cost Is: Out-of-Network Benefits Your Cost Is: Office, health center, and home medical services by another specialist or other covered provider (non-hospital), including a physician assistant or nurse practitioner designated by the health plan as specialty care $40 copayment per visit after deductible 20% after deductible Hospital outpatient medical services $40 copayment per visit after deductible 20% after deductible Medical Care Outpatient Visits (continued) Acupuncture services (12-visit benefit limit per member per calendar year) $40 copayment per visit after deductible 20% after deductible Medical Formulas Certain medical formulas and low protein foods See Prescription Drugs and Supplies See Prescription Drugs and Supplies Inpatient admissions in a General Hospital Hospital services No charge after deductible 20% after deductible Physician and other covered professional provider services No charge after deductible 20% after deductible Inpatient admissions in a Mental Hospital or Substance Use Facility Facility services No charge after deductible 20% after deductible Physician and other covered professional provider services No charge after deductible 20% after deductible Mental Health and Substance Use Treatment Outpatient services $25 copayment per visit after deductible 20% after deductible Oxygen and equipment for its administration No charge after deductible 20% after deductible Oxygen and Respiratory Therapy Outpatient respiratory therapy See Medical Care Outpatient Visits See Medical Care Outpatient Visits Outpatient lab tests and x-rays See Lab Tests, X-Rays, and Other Tests See Lab Tests, X-Rays, and Other Tests Outpatient surgical services See Surgery as an Outpatient See Surgery as an Outpatient Podiatry Care Outpatient medical care services See Medical Care Outpatient Visits See Medical Care Outpatient Visits
 Blue Cross Blue Shield of Massachusetts Subscriber Information Page 132 Page 134
Blue Cross Blue Shield of Massachusetts Subscriber Information Page 132 Page 134