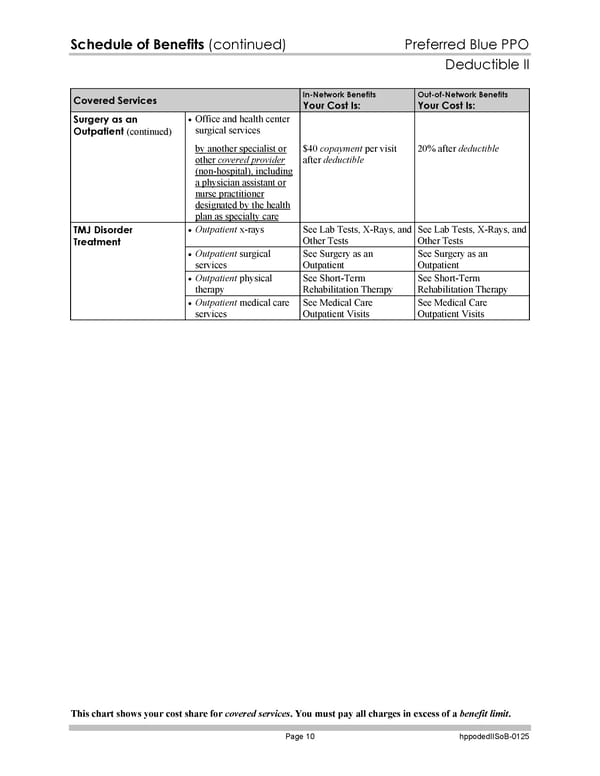
Schedule of Benefits (continued) Preferred Blue PPO Deductible II This chart shows your cost share for covered services. You must pay all charges in excess of a benefit limit. Page 10 hppodedIISoB-0125 Covered Services In-Network Benefits Your Cost Is: Out-of-Network Benefits Your Cost Is: Office and health center surgical services Surgery as an Outpatient (continued) by another specialist or other covered provider (non-hospital), including a physician assistant or nurse practitioner designated by the health plan as specialty care $40 copayment per visit after deductible 20% after deductible Outpatient x-rays See Lab Tests, X-Rays, and Other Tests See Lab Tests, X-Rays, and Other Tests Outpatient surgical services See Surgery as an Outpatient See Surgery as an Outpatient Outpatient physical therapy See Short-Term Rehabilitation Therapy See Short-Term Rehabilitation Therapy TMJ Disorder Treatment Outpatient medical care services See Medical Care Outpatient Visits See Medical Care Outpatient Visits
 Blue Cross Blue Shield of Massachusetts Subscriber Information Page 136 Page 138
Blue Cross Blue Shield of Massachusetts Subscriber Information Page 136 Page 138