Harvard Pilgrim Healthcare Waiver Form
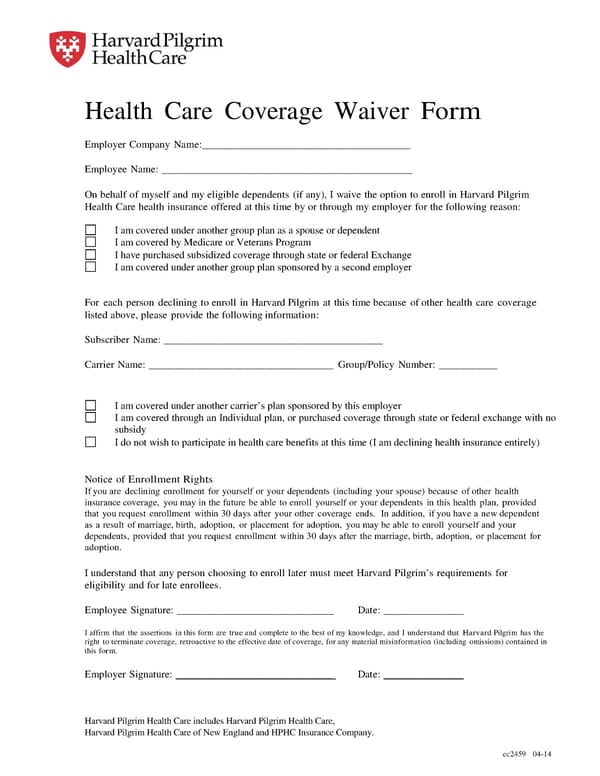
Health Care Coverage Waiver Form Employer Company Name:_______________________________________ Employee Name: _______________________________________________ On behalf of myself and my eligible dependents (if any), I waive the option to enroll in Harvard Pilgrim Health Care health insurance offered at this time by or through my employer for the following reason: I am covered under another group plan as a spouse or dependent I am covered by Medicare or Veterans Program I have purchased subsidized coverage through state or federal Exchange I am covered under another group plan sponsored by a second employer For each person declining to enroll in Harvard Pilgrim at this time because of other health care coverage listed above, please provide the following information: Subscriber Name: _________________________________________ ___________________________________ Group/Policy Number: ___________ Carrier Name: I am covered under another carrier’s plan sponsored by this employer I am covered through an Individual plan, or purchased coverage through state or federal exchange with no subsidy I do not wish to participate in health care benefits at this time (I am declining health insurance entirely) No Enrollment Rights tice of If you are declining enrollment for yourself or your dependents (including your spouse) because of other health insurance coverage, you may in the future be able to enroll yourself or your dependents in this health plan, provided that you request enrollment within 30 days after your other coverage ends. In addition, if you have a new dependent as a result of marriage, birth, adoption, or placement for adoption, you may be able to enroll yourself and your dependents, provided that you request enrollment within 30 days after the marriage, birth, adoption, or placement for adoption. I understand that any person choosing to enroll later must meet Harvard Pilgrim’s requirements for eligibility and for late enrollees. _______________ Employee Signature: ______________________________ Date: I affirm that the assertions in this form are true and complete to the best of my knowledge, and I understand that Harvard Pilgrim has the right to terminate coverage, retroactive to the effective date of coverage, for any material misinformation (including omissions) contained in this form. Employer Signature: ______________________________ Date: _______________ Harvard Pilgrim Health Care includes Harvard Pilgrim Health Care, Harvard Pilgrim Health Care of New England and HPHC Insurance Company. cc2459 04-14
 Harvard Pilgrim Healthcare Waiver Form
Harvard Pilgrim Healthcare Waiver Form