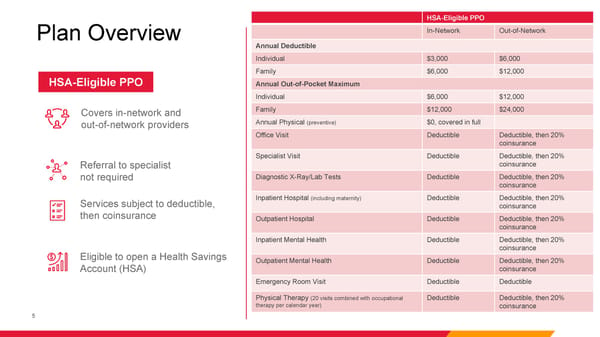
HSA-Eligible PPO Plan Overview In-Network Out-of-Network Annual Deductible Individual $3,000 $6,000 Family $6,000 $12,000 HSA-Eligible PPO Annual Out-of-Pocket Maximum Individual $6,000 $12,000 Covers in-network and Family $12,000 $24,000 out-of-network providers Annual Physical (preventive) $0, covered in full Office Visit Deductible Deductible, then 20% coinsurance Specialist Visit Deductible Deductible, then 20% Referral to specialist coinsurance not required Diagnostic X-Ray/Lab Tests Deductible Deductible, then 20% coinsurance Services subject to deductible, Inpatient Hospital (including maternity) Deductible Deductible, then 20% coinsurance then coinsurance Outpatient Hospital Deductible Deductible, then 20% coinsurance Inpatient Mental Health Deductible Deductible, then 20% Eligible to open a Health Savings coinsurance Outpatient Mental Health Deductible Deductible, then 20% Account (HSA) coinsurance Emergency Room Visit Deductible Deductible Physical Therapy (20 visits combined with occupational Deductible Deductible, then 20% therapy per calendar year) coinsurance 5
 HPHC Additional Resources Page 4 Page 6
HPHC Additional Resources Page 4 Page 6