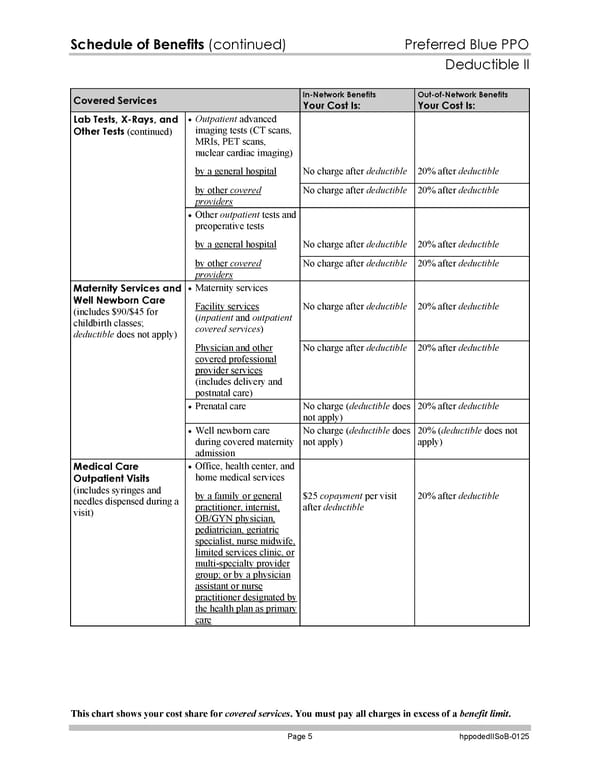
Schedule of Benefits (continued) Preferred Blue PPO Deductible II This chart shows your cost share for covered services. You must pay all charges in excess of a benefit limit. Page 5 hppodedIISoB-0125 Covered Services In-Network Benefits Your Cost Is: Out-of-Network Benefits Your Cost Is: Outpatient advanced imaging tests (CT scans, MRIs, PET scans, nuclear cardiac imaging) by a general hospital No charge after deductible 20% after deductible by other covered providers No charge after deductible 20% after deductible Other outpatient tests and preoperative tests by a general hospital No charge after deductible 20% after deductible Lab Tests, X-Rays, and Other Tests (continued) by other covered providers No charge after deductible 20% after deductible Maternity services Facility services (inpatient and outpatient covered services) No charge after deductible 20% after deductible Physician and other covered professional provider services (includes delivery and postnatal care) No charge after deductible 20% after deductible Prenatal care No charge (deductible does not apply) 20% after deductible Maternity Services and Well Newborn Care (includes $90/$45 for childbirth classes; deductible does not apply) Well newborn care during covered maternity admission No charge (deductible does not apply) 20% (deductible does not apply) Office, health center, and home medical services Medical Care Outpatient Visits (includes syringes and needles dispensed during a visit) by a family or general practitioner, internist, OB/GYN physician, pediatrician, geriatric specialist, nurse midwife, limited services clinic, or multi-specialty provider group; or by a physician assistant or nurse practitioner designated by the health plan as primary care $25 copayment per visit after deductible 20% after deductible
 Subscriber Certificate and Rider Documentation Page 131 Page 133
Subscriber Certificate and Rider Documentation Page 131 Page 133