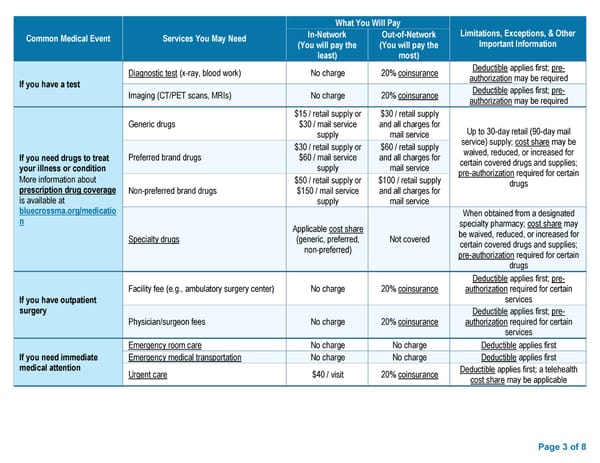
What You Will Pay Common Medical Event Services You May Need In-Network Out-of-Network Limitations, Exceptions, & Other (You will pay the (You will pay the Important Information least) most) Diagnostic test (x-ray, blood work) No charge 20% coinsurance Deductible applies first; pre- If you have a test authorization may be required Imaging (CT/PET scans, MRIs) No charge 20% coinsurance Deductible applies first; pre- authorization may be required $15 / retail supply or $30 / retail supply Generic drugs $30 / mail service and all charges for Up to 30-day retail (90-day mail supply mail service service) supply; cost share may be $30 / retail supply or $60 / retail supply waived, reduced, or increased for If you need drugs to treat Preferred brand drugs $60 / mail service and all charges for certain covered drugs and supplies; your illness or condition supply mail service pre-authorization required for certain More information about $50 / retail supply or $100 / retail supply drugs prescription drug coverage Non-preferred brand drugs $150 / mail service and all charges for is available at supply mail service bluecrossma.org/medicatio When obtained from a designated n Applicable cost share specialty pharmacy; cost share may Specialty drugs (generic, preferred, Not covered be waived, reduced, or increased for non-preferred) certain covered drugs and supplies; pre-authorization required for certain drugs Deductible applies first; pre- Facility fee (e.g., ambulatory surgery center) No charge 20% coinsurance authorization required for certain If you have outpatient services surgery Deductible applies first; pre- Physician/surgeon fees No charge 20% coinsurance authorization required for certain services Emergency room care No charge No charge Deductible applies first If you need immediate Emergency medical transportation No charge No charge Deductible applies first medical attention Urgent care $40 / visit 20% coinsurance Deductible applies first; a telehealth cost share may be applicable Page 3 of 8
 Summary of Benefits and Coverage - Preferred Blue PPO $4000 Deductible II Page 2 Page 4
Summary of Benefits and Coverage - Preferred Blue PPO $4000 Deductible II Page 2 Page 4