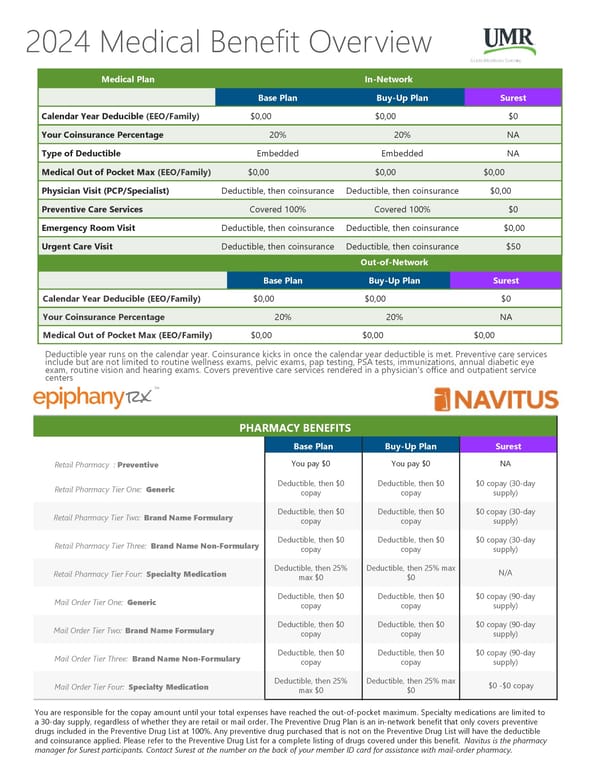
2024 Medical Benefit Overview Medical Plan In-Network Base Plan Buy-Up Plan Surest Calendar Year Deducible (EEO/Family) $0,00 $0,00 $0 Your Coinsurance Percentage 20% 20% NA Type of Deductible Embedded Embedded NA Medical Out of Pocket Max (EEO/Family) $0,00 $0,00 $0,00 Physician Visit (PCP/Specialist) Deductible, then coinsurance Deductible, then coinsurance $0,00 Preventive Care Services Covered 100% Covered 100% $0 Emergency Room Visit Deductible, then coinsurance Deductible, then coinsurance $0,00 Urgent Care Visit Deductible, then coinsurance Deductible, then coinsurance $50 Out-of-Network Base Plan Buy-Up Plan Surest Calendar Year Deducible (EEO/Family) $0,00 $0,00 $0 Your Coinsurance Percentage 20% 20% NA Medical Out of Pocket Max (EEO/Family) $0,00 $0,00 $0,00 Deductible year runs on the calendar year. Coinsurance kicks in once the calendar year deductible is met. Preventive care services include but are not limited to routine wellness exams, pelvic exams, pap testing, PSA tests, immunizations, annual diabetic eye exam, routine vision and hearing exams. Covers preventive care services rendered in a physician's office and outpatient service centers PHARMACY BENEFITS Base Plan Buy-Up Plan Surest Retail Pharmacy : Preventive You pay $0 You pay $0 NA Retail Pharmacy Tier One: Generic Deductible, then $0 Deductible, then $0 $0 copay (30-day copay copay supply) Retail Pharmacy Tier Two: Brand Name Formulary Deductible, then $0 Deductible, then $0 $0 copay (30-day copay copay supply) Retail Pharmacy Tier Three: Brand Name Non-Formulary Deductible, then $0 Deductible, then $0 $0 copay (30-day copay copay supply) Retail Pharmacy Tier Four: Specialty Medication Deductible, then 25% Deductible, then 25% max N/A max $0 $0 Mail Order Tier One: Generic Deductible, then $0 Deductible, then $0 $0 copay (90-day copay copay supply) Mail Order Tier Two: Brand Name Formulary Deductible, then $0 Deductible, then $0 $0 copay (90-day copay copay supply) Mail Order Tier Three: Brand Name Non-Formulary Deductible, then $0 Deductible, then $0 $0 copay (90-day copay copay supply) Mail Order Tier Four: Specialty Medication Deductible, then 25% Deductible, then 25% max $0 -$0 copay max $0 $0 You are responsible for the copay amount until your total expenses have reached the out-of-pocket maximum. Specialty medications are limited to a 30-day supply, regardless of whether they are retail or mail order. The Preventive Drug Plan is an in-network benefit that only covers preventive drugs included in the Preventive Drug List at 100%. Any preventive drug purchased that is not on the Preventive Drug List will have the deductible and coinsurance applied. Please refer to the Preventive Drug List for a complete listing of drugs covered under this benefit. Navitus is the pharmacy manager for Surest participants. Contact Surest at the number on the back of your member ID card for assistance with mail-order pharmacy.
 2024 Cobra Benefits Guide Page 4 Page 6
2024 Cobra Benefits Guide Page 4 Page 6