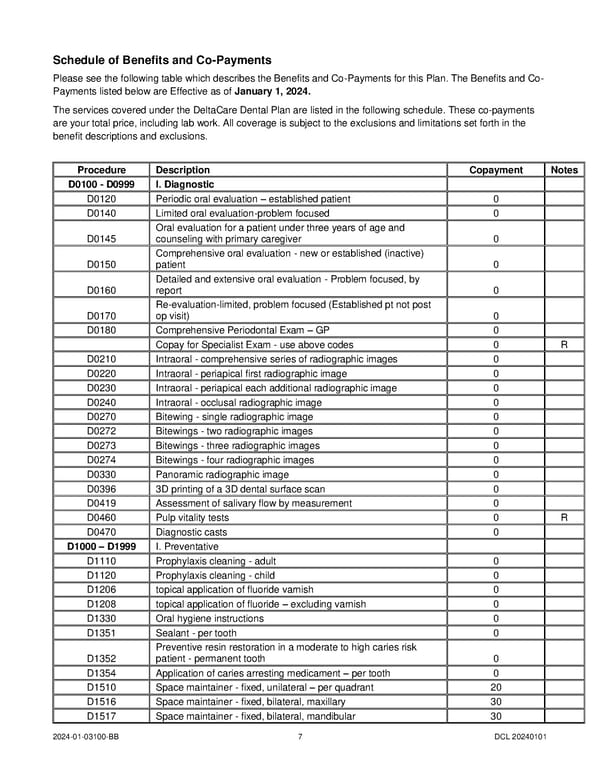
Schedule of Benefits and Co-Payments Please see the following table which describes the Benefits and Co-Payments for this Plan. The Benefits and Co- Payments listed below are Effective as of January 1, 2024. The services covered under the DeltaCare Dental Plan are listed in the following schedule. These co-payments are your total price, including lab work. All coverage is subject to the exclusions and limitations set forth in the benefit descriptions and exclusions. Procedure Description Copayment Notes D0100 - D0999 I. Diagnostic D0120 Periodic oral evaluation – established patient 0 D0140 Limited oral evaluation-problem focused 0 Oral evaluation for a patient under three years of age and D0145 counseling with primary caregiver 0 Comprehensive oral evaluation - new or established (inactive) D0150 patient 0 Detailed and extensive oral evaluation - Problem focused, by D0160 report 0 Re-evaluation-limited, problem focused (Established pt not post D0170 op visit) 0 D0180 Comprehensive Periodontal Exam – GP 0 Copay for Specialist Exam - use above codes 0 R D0210 Intraoral - comprehensive series of radiographic images 0 D0220 Intraoral - periapical first radiographic image 0 D0230 Intraoral - periapical each additional radiographic image 0 D0240 Intraoral - occlusal radiographic image 0 D0270 Bitewing - single radiographic image 0 D0272 Bitewings - two radiographic images 0 D0273 Bitewings - three radiographic images 0 D0274 Bitewings - four radiographic images 0 D0330 Panoramic radiographic image 0 D0396 3D printing of a 3D dental surface scan 0 D0419 Assessment of salivary flow by measurement 0 D0460 Pulp vitality tests 0 R D0470 Diagnostic casts 0 D1000 – D1999 I. Preventative D1110 Prophylaxis cleaning - adult 0 D1120 Prophylaxis cleaning - child 0 D1206 topical application of fluoride varnish 0 D1208 topical application of fluoride – excluding varnish 0 D1330 Oral hygiene instructions 0 D1351 Sealant - per tooth 0 Preventive resin restoration in a moderate to high caries risk D1352 patient - permanent tooth 0 D1354 Application of caries arresting medicament – per tooth 0 D1510 Space maintainer - fixed, unilateral – per quadrant 20 D1516 Space maintainer - fixed, bilateral, maxillary 30 D1517 Space maintainer - fixed, bilateral, mandibular 30 2024-01-03100-BB 7 DCL 20240101
 DeltaCare COC (2024) Page 10 Page 12
DeltaCare COC (2024) Page 10 Page 12