Open Enrollment Template | with audio recording
Template developed by Meridian Software Services
Company Name Open Enrollment 2023

Table of Contents Welcome to Open Enrollment 3 Benefits Overview 7 Medical Overview 9 Dental Overview 15 Vision Overview 17 Life Insurance Overview 19 Disability Overview 21 Financial Overview 23 Perks at Work 27 Questions & Answers 29
Welcome to Open Enrollment

Eligibility & Qualifying Events Eligibility Qualifying Events The elections you make during open All full-time employees working 30 enrollment will remain in place for the entire hours or more per week are eligible to year, unless you have a qualifying event. enroll in the benefit programs. Qualifying events include: You can cover: Spouse Marriage/Legal Separation/Divorce Dependent Children Birth of a Child/Adoption Loss of Other Coverage
This is a modal window.
Open Enrollment Period November 11, 2023 – November 29, 2023 Open Enrollment Timeline January 1, 2023 – December 31, 2023 Plan Effective Dates Enrollment Portal
This is a modal window.
Meet Alex
Benefits Overview
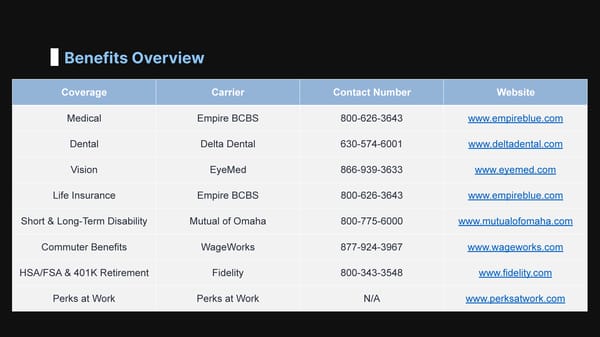
Benefits Overview Coverage Carrier Contact Number Website Medical Empire BCBS 800-626-3643 www.empireblue.com Dental Delta Dental 630-574-6001 www.deltadental.com Vision EyeMed 866-939-3633 www.eyemed.com Life Insurance Empire BCBS 800-626-3643 www.empireblue.com Short & Long-Term Disability Mutual of Omaha 800-775-6000 www.mutualofomaha.com Commuter Benefits WageWorks 877-924-3967 www.wageworks.com HSA/FSA & 401K Retirement Fidelity 800-343-3548 www.fidelity.com Perks at Work Perks at Work N/A www.perksatwork.com
Key Terms Annual Deductible Embedded | Aggregate Out-Of-Pocket Maximum Embedded | Aggregate Copay / Coinsurance Copay | Coinsurance

This is a modal window.
Preventative Care You are eligible to receive certain preventative and wellness services at no cost. Medical No cost means: • No Deductible • No Copays Overview • No Coinsurance
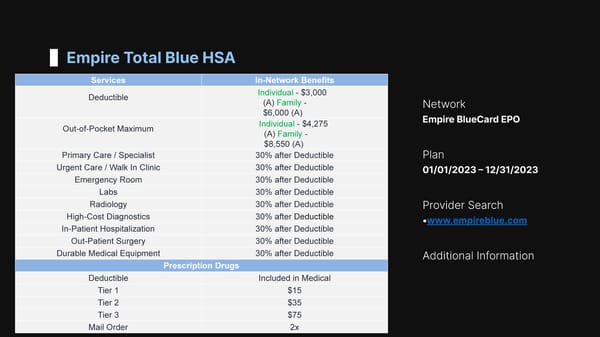
Empire Total Blue HSA Services In-Network Benefits Individual - $3,000 Deductible (A) Family - Network $6,000 (A) Empire BlueCard EPO Individual - $4,275 Out-of-Pocket Maximum (A) Family - $8,550 (A) Primary Care / Specialist 30% after Deductible Plan Urgent Care / Walk In Clinic 30% after Deductible 01/01/2023 – 12/31/2023 Emergency Room 30% after Deductible Labs 30% after Deductible Radiology 30% after Deductible Provider Search High-Cost Diagnostics 30% after Deductible •www.empireblue.com In-Patient Hospitalization 30% after Deductible Out-Patient Surgery 30% after Deductible Durable Medical Equipment 30% after Deductible Additional Information Prescription Drugs Deductible Included in Medical Tier 1 $15 Tier 2 $35 Tier 3 $75 Mail Order 2x
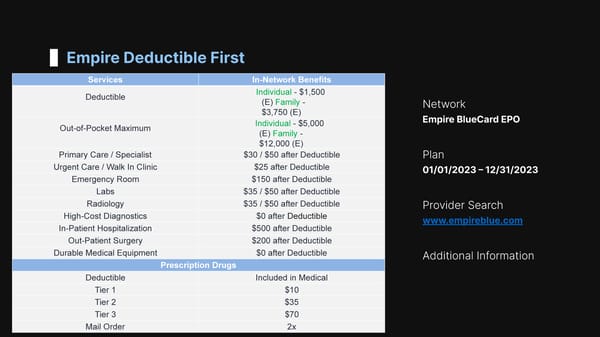
Empire Deductible First Services In-Network Benefits Individual - $1,500 Deductible (E) Family - Network $3,750 (E) Empire BlueCard EPO Individual - $5,000 Out-of-Pocket Maximum (E) Family - $12,000 (E) Primary Care / Specialist $30 / $50 after Deductible Plan Urgent Care / Walk In Clinic $25 after Deductible 01/01/2023 – 12/31/2023 Emergency Room $150 after Deductible Labs $35 / $50 after Deductible Radiology $35 / $50 after Deductible Provider Search High-Cost Diagnostics $0 after Deductible www.empireblue.com In-Patient Hospitalization $500 after Deductible Out-Patient Surgery $200 after Deductible Durable Medical Equipment $0 after Deductible Additional Information Prescription Drugs Deductible Included in Medical Tier 1 $10 Tier 2 $35 Tier 3 $70 Mail Order 2x
Telemedicine Visit board certified providers 24/7 from your phone, tablet or computer Medical Services Psychology Counseling Services Cost
This is a modal window.
Sidney App

Additional Benefits You must be enrolled in Empire Medical for these additional benefits. Life Insurance Life & AD&D Insurance = $25,000 Make sure your beneficiary designation is up to date! 1 Vision Insurance 1 eye exam every 24 months for $15 copay 2 Employee Assistance Counseling, Financial Planning, Legal Support, 3 ID theft recovery, Beneficiary support
This is a modal window.
Dental Overview

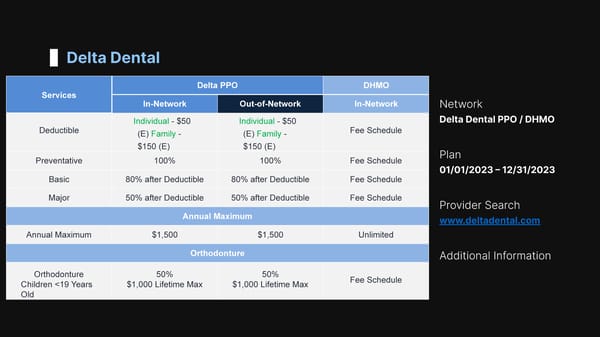
Delta Dental Delta PPO DHMO Services In-Network Out-of-Network In-Network Network Delta Dental PPO / DHMO Individual - $50 Individual - $50 Deductible Fee Schedule (E) Family - (E) Family - $150 (E) $150 (E) Plan Preventative 100% 100% Fee Schedule 01/01/2023 – 12/31/2023 Basic 80% after Deductible 80% after Deductible Fee Schedule Major 50% after Deductible 50% after Deductible Fee Schedule Provider Search Annual Maximum www.deltadental.com Annual Maximum $1,500 $1,500 Unlimited Orthodonture Additional Information Orthodonture 50% 50% Fee Schedule Children
Vision Overview

EyeMed Vision EyeMed Services Network Frequency Benefit Out-of-Network EyeMed Exam 12 Months $20 $40 Reimbursement Prescription Glasses Plan $100 Allowance + 01/01/2023 – 12/31/2023 Eyeglass Frames 24 Months $75 Reimbursement 20% Discount on Balance Eyeglass Lenses Provider Search $30 / $50 / $70 www.eyemed.com Single / Bifocal / Trifocal 24 Months $20 Reimbursement Contact Lenses Additional Information $100 Allowance + Elective 24 Months $100 Reimbursement 15% Discount on Balance Medically Necessary 12 Months Covered 100% $210 Reimbursement

Life Insurance Overview

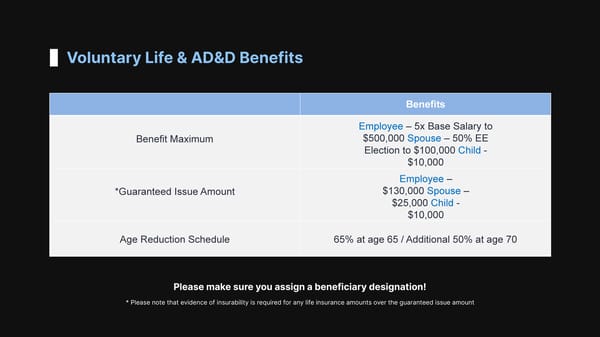
Voluntary Life & AD&D Benefits Benefits Employee – 5x Base Salary to $500,000 Spouse – 50% EE Benefit Maximum Election to $100,000 Child - $10,000 Employee – $130,000 Spouse – *Guaranteed Issue Amount $25,000 Child - $10,000 Age Reduction Schedule 65% at age 65 / Additional 50% at age 70 Please make sure you assign a beneficiary designation! * Please note that evidence of insurability is required for any life insurance amounts over the guaranteed issue amount
Disability Overview

Voluntary STD / LTD Benefits Long-Term Disability Short-Term Disability Benefits Benefits th st Benefits Start 8 Day Accident / Illness Benefits Start 91 Day of Disability Benefit Duration Up to 13 Weeks Benefit Duration Up to SSNRA Percentage of Income Percentage of Income 60% 60% Replacement Replacement Benefit Maximum $1,500 Per Week Benefit Maximum $5,000 Per Month * Please note if you have previously waived participation in the * Please note the STD benefit is offered on an annual LTD benefits and would like to enroll during open enrollment, you enrollment basis, so you can elect this benefit will need to submit evidence of insurability to Mutual of Omaha even if you have previously waived participation

Financial Overview

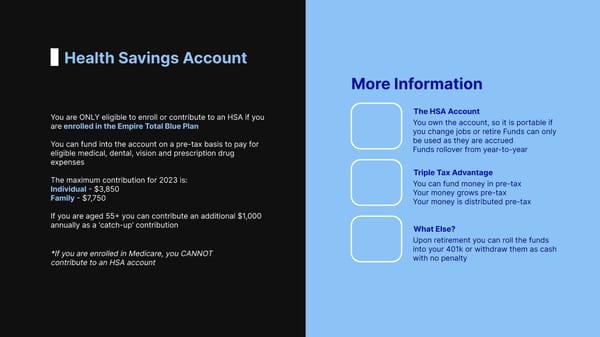
Health Savings Account More Information The HSA Account You are ONLY eligible to enroll or contribute to an HSA if you You own the account, so it is portable if are enrolled in the Empire Total Blue Plan you change jobs or retire Funds can only be used as they are accrued You can fund into the account on a pre-tax basis to pay for Funds rollover from year-to-year eligible medical, dental, vision and prescription drug expenses Triple Tax Advantage The maximum contribution for 2023 is: You can fund money in pre-tax Individual - $3,850 Your money grows pre-tax Family - $7,750 Your money is distributed pre-tax If you are aged 55+ you can contribute an additional $1,000 annually as a ‘catch-up’ contribution What Else? Upon retirement you can roll the funds into your 401k or withdraw them as cash *If you are enrolled in Medicare, you CANNOT with no penalty contribute to an HSA account
Flexible Spending Accounts Flexible Spending Account • You can fund into the account on a pre-tax basis to pay for eligible medical, dental, vision and prescription drug expenses • The maximum contribution for 2023 is $3,050 • Funds are available on the 1st day of the plan year • You can rollover up to $500 ofunused funds into the 2023 plan year • If you are enrolled in the health savings account, your flexible spending account would become ‘limited purpose’ meaning it can only be used for eligible dental and vision expenses Triple Tax Advantage • You can fund into the account on a pre-tax basis to pay for eligible dependent care expenses • The maximum contribution for 2023 is $5,000 • Funds are only available as you accrue them • Funds are ‘use it or lose it’

This is a modal window.
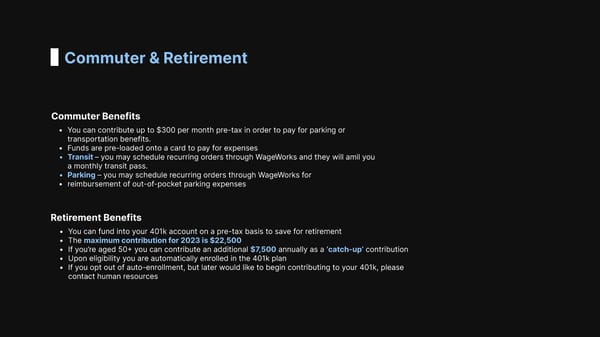
Commuter & Retirement Commuter Benefits • You can contribute up to $300 per month pre-tax in order to pay for parking or transportation benefits. • Funds are pre-loaded onto a card to pay for expenses • Transit – you may schedule recurring orders through WageWorks and they will amil you a monthly transit pass. • Parking – you may schedule recurring orders through WageWorks for • reimbursement of out-of-pocket parking expenses Retirement Benefits • You can fund into your 401k account on a pre-tax basis to save for retirement • The maximum contribution for 2023 is $22,500 • If you’re aged 50+ you can contribute an additional $7,500 annually as a ‘catch-up’ contribution • Upon eligibility you are automatically enrolled in the 401k plan • If you opt out of auto-enrollment, but later would like to begin contributing to your 401k, please contact human resources
This is a modal window.
Perks at Work Overview
Perks at Work
Q & A What Should You Do? Step 1 Step 3 Complete You Selections by 11/29/2022 Review Your Renewal Options Step 2 Step 4 Login and Make Your Selections in Paycom. Plans are Effective 01/01/2023 – 12/31/2023
Your Agency Team Name 02 Name 03 Name 01 Account VIP Customer Lead Management Service Consultant
Contact Us 123-456-7890 Website Location Email