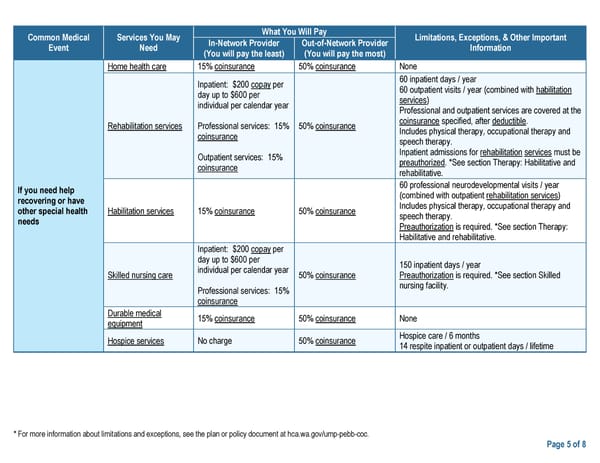
Common Medical Services You May What You Will Pay Limitations, Exceptions, & Other Important Event Need In-Network Provider Out-of-Network Provider Information (You will pay the least) (You will pay the most) Home health care 15% coinsurance 50% coinsurance None Inpatient: $200 copay per 60 inpatient days / year day up to $600 per 60 outpatient visits / year (combined with habilitation individual per calendar year services) Professional and outpatient services are covered at the Rehabilitation services Professional services: 15% 50% coinsurance coinsurance specified, after deductible. coinsurance Includes physical therapy, occupational therapy and speech therapy. Outpatient services: 15% Inpatient admissions for rehabilitation services must be coinsurance preauthorized. *See section Therapy: Habilitative and rehabilitative. If you need help 60 professional neurodevelopmental visits / year recovering or have (combined with outpatient rehabilitation services) other special health Habilitation services 15% coinsurance 50% coinsurance Includes physical therapy, occupational therapy and needs speech therapy. Preauthorization is required. *See section Therapy: Habilitative and rehabilitative. Inpatient: $200 copay per day up to $600 per 150 inpatient days / year Skilled nursing care individual per calendar year 50% coinsurance Preauthorization is required. *See section Skilled Professional services: 15% nursing facility. coinsurance Durable medical 15% coinsurance 50% coinsurance None equipment Hospice services No charge 50% coinsurance Hospice care / 6 months 14 respite inpatient or outpatient days / lifetime * For more information about limitations and exceptions, see the plan or policy document at hca.wa.gov/ump-pebb-coc. Page 5 of 8
 UMP Plus–Puget Sound High Value Network (PSHVN) SBC (2024) Page 4 Page 6
UMP Plus–Puget Sound High Value Network (PSHVN) SBC (2024) Page 4 Page 6