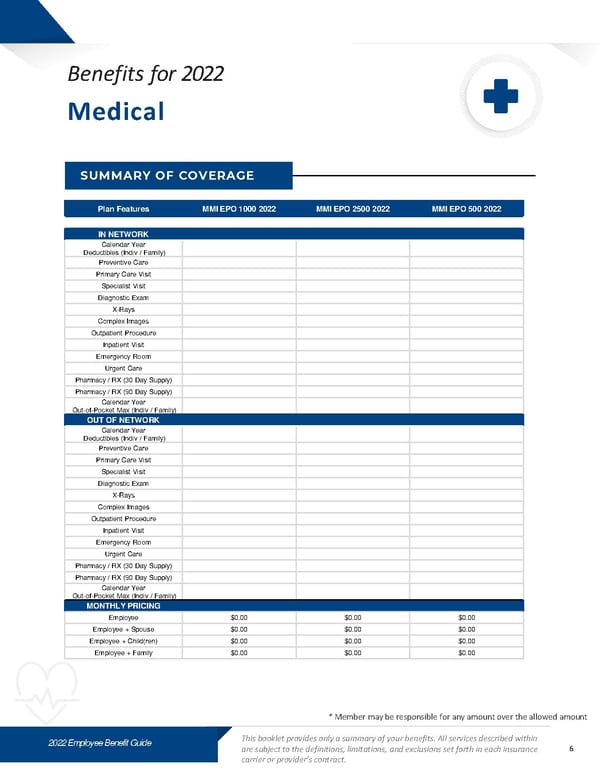
2022 Employee Benefit Guide This booklet provides only a summary of your benefits. All services described within are subject to the definitions, limitations, and exclusions set forth in each insurance carrier or provider’s contract. Plan Features MMI EPO 1000 202 2 MMI EPO 2500 2022 MMI EPO 500 202 2 IN NETWORK Calendar Year Deductibles (Indiv / Family) Preventive Care Primary Care Visit Specialist Visit Diagnostic Exam X - Rays Complex Images Outpatient Procedure Inpatient Visit Emergency Room Urgent Care Pharmacy / RX (30 Day Supply) Pharmacy / RX (90 Day Supply) Calendar Year Out - of - Pocket Max (Indiv / Family) OUT OF NETWORK Calendar Year Deductibles (Indiv / Family) Preventive Care Primary Care Visit Specialist Visit Diagnostic Exam X - Rays Complex Images Outpatient Procedure Inpatient Visit Emergency Room Urgent Care Pharmacy / RX (30 Day Supply) Pharmacy / RX (90 Day Supply) Calendar Year Out - of - Pocket Max (Indiv / Family) MONTHLY PRICING Employee $0.00 $0.00 $0.00 Employee + Spouse $0.00 $0.00 $0.00 Employee + Child(ren) $0.00 $0.00 $0.00 Employee + Family $0.00 $0.00 $0.00 * Member may be responsible for any amount over the allowed amount Benefits f or 2022 SUMMARY OF COVERAGE Medical 6
 Benefits Guide - Contemporary Style Template Page 5 Page 7
Benefits Guide - Contemporary Style Template Page 5 Page 7