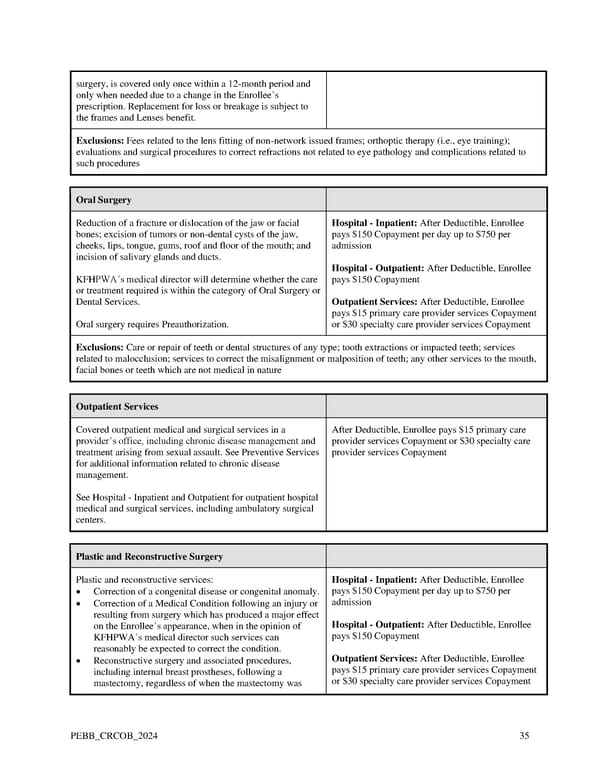
surgery, is covered only once within a 12-month period and only when needed due to a change in the Enrollee’s prescription. Replacement for loss or breakage is subject to the frames and Lenses benefit. Exclusions: Fees related to the lens fitting of non-network issued frames; orthoptic therapy (i.e., eye training); evaluations and surgical procedures to correct refractions not related to eye pathology and complications related to such procedures Oral Surgery Reduction of a fracture or dislocation of the jaw or facial Hospital - Inpatient: After Deductible, Enrollee bones; excision of tumors or non-dental cysts of the jaw, pays $150 Copayment per day up to $750 per cheeks, lips, tongue, gums, roof and floor of the mouth; and admission incision of salivary glands and ducts. Hospital - Outpatient: After Deductible, Enrollee KFHPWA’s medical director will determine whether the care pays $150 Copayment or treatment required is within the category of Oral Surgery or Dental Services. Outpatient Services: After Deductible, Enrollee pays $15 primary care provider services Copayment Oral surgery requires Preauthorization. or $30 specialty care provider services Copayment Exclusions: Care or repair of teeth or dental structures of any type; tooth extractions or impacted teeth; services related to malocclusion; services to correct the misalignment or malposition of teeth; any other services to the mouth, facial bones or teeth which are not medical in nature Outpatient Services Covered outpatient medical and surgical services in a After Deductible, Enrollee pays $15 primary care provider’s office, including chronic disease management and provider services Copayment or $30 specialty care treatment arising from sexual assault. See Preventive Services provider services Copayment for additional information related to chronic disease management. See Hospital - Inpatient and Outpatient for outpatient hospital medical and surgical services, including ambulatory surgical centers. Plastic and Reconstructive Surgery Plastic and reconstructive services: Hospital - Inpatient: After Deductible, Enrollee • Correction of a congenital disease or congenital anomaly. pays $150 Copayment per day up to $750 per • Correction of a Medical Condition following an injury or admission resulting from surgery which has produced a major effect on the Enrollee’s appearance, when in the opinion of Hospital - Outpatient: After Deductible, Enrollee KFHPWA’s medical director such services can pays $150 Copayment reasonably be expected to correct the condition. • Reconstructive surgery and associated procedures, Outpatient Services: After Deductible, Enrollee including internal breast prostheses, following a pays $15 primary care provider services Copayment mastectomy, regardless of when the mastectomy was or $30 specialty care provider services Copayment PEBB_CRCOB_2024 35
 Kaiser Permanente WA Original Medicare EOC (2024) Page 34 Page 36
Kaiser Permanente WA Original Medicare EOC (2024) Page 34 Page 36