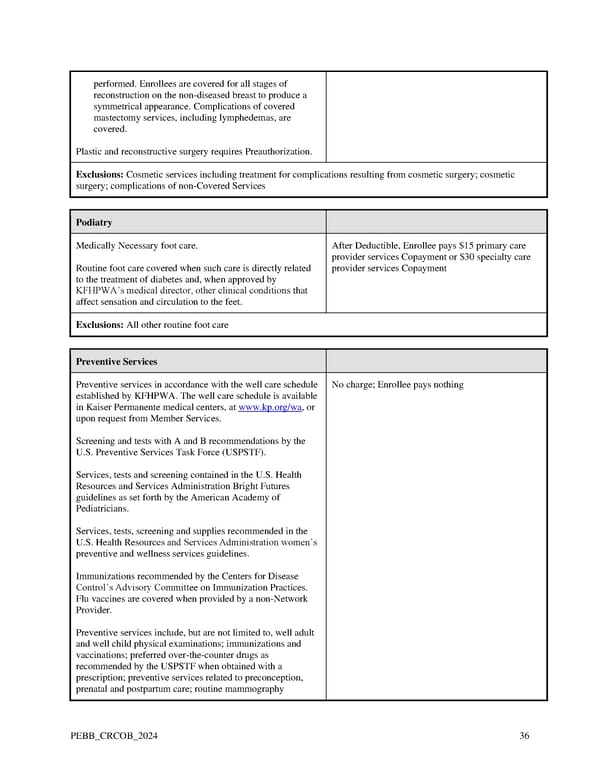
performed. Enrollees are covered for all stages of reconstruction on the non-diseased breast to produce a symmetrical appearance. Complications of covered mastectomy services, including lymphedemas, are covered. Plastic and reconstructive surgery requires Preauthorization. Exclusions: Cosmetic services including treatment for complications resulting from cosmetic surgery; cosmetic surgery; complications of non-Covered Services Podiatry Medically Necessary foot care. After Deductible, Enrollee pays $15 primary care provider services Copayment or $30 specialty care Routine foot care covered when such care is directly related provider services Copayment to the treatment of diabetes and, when approved by KFHPWA’s medical director, other clinical conditions that affect sensation and circulation to the feet. Exclusions: All other routine foot care Preventive Services Preventive services in accordance with the well care schedule No charge; Enrollee pays nothing established by KFHPWA. The well care schedule is available in Kaiser Permanente medical centers, at www.kp.org/wa, or upon request from Member Services. Screening and tests with A and B recommendations by the U.S. Preventive Services Task Force (USPSTF). Services, tests and screening contained in the U.S. Health Resources and Services Administration Bright Futures guidelines as set forth by the American Academy of Pediatricians. Services, tests, screening and supplies recommended in the U.S. Health Resources and Services Administration women’s preventive and wellness services guidelines. Immunizations recommended by the Centers for Disease Control’s Advisory Committee on Immunization Practices. Flu vaccines are covered when provided by a non-Network Provider. Preventive services include, but are not limited to, well adult and well child physical examinations; immunizations and vaccinations; preferred over-the-counter drugs as recommended by the USPSTF when obtained with a prescription; preventive services related to preconception, prenatal and postpartum care; routine mammography PEBB_CRCOB_2024 36
 Kaiser Permanente WA Original Medicare EOC (2024) Page 35 Page 37
Kaiser Permanente WA Original Medicare EOC (2024) Page 35 Page 37