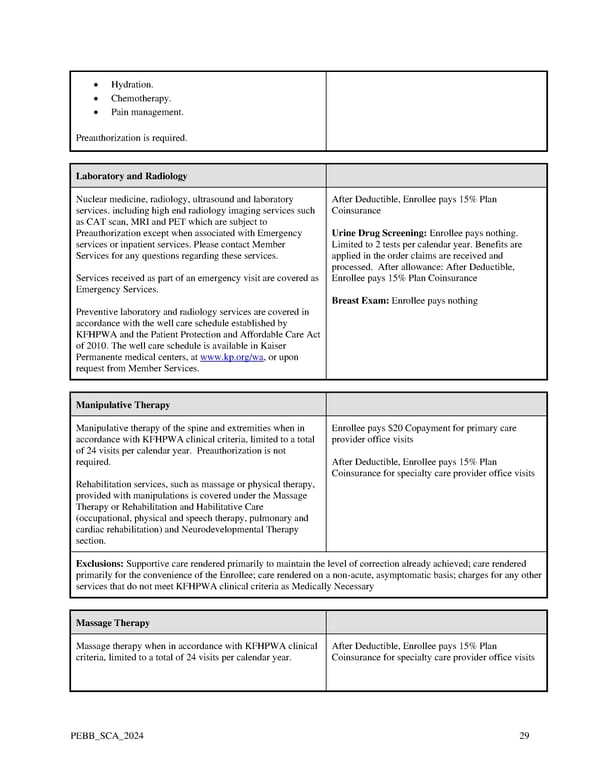
• Hydration. • Chemotherapy. • Pain management. Preauthorization is required. Laboratory and Radiology Nuclear medicine, radiology, ultrasound and laboratory After Deductible, Enrollee pays 15% Plan services. including high end radiology imaging services such Coinsurance as CAT scan, MRI and PET which are subject to Preauthorization except when associated with Emergency Urine Drug Screening: Enrollee pays nothing. services or inpatient services. Please contact Member Limited to 2 tests per calendar year. Benefits are Services for any questions regarding these services. applied in the order claims are received and processed. After allowance: After Deductible, Services received as part of an emergency visit are covered as Enrollee pays 15% Plan Coinsurance Emergency Services. Breast Exam: Enrollee pays nothing Preventive laboratory and radiology services are covered in accordance with the well care schedule established by KFHPWA and the Patient Protection and Affordable Care Act of 2010. The well care schedule is available in Kaiser Permanente medical centers, at www.kp.org/wa, or upon request from Member Services. Manipulative Therapy Manipulative therapy of the spine and extremities when in Enrollee pays $20 Copayment for primary care accordance with KFHPWA clinical criteria, limited to a total provider office visits of 24 visits per calendar year. Preauthorization is not required. After Deductible, Enrollee pays 15% Plan Coinsurance for specialty care provider office visits Rehabilitation services, such as massage or physical therapy, provided with manipulations is covered under the Massage Therapy or Rehabilitation and Habilitative Care (occupational, physical and speech therapy, pulmonary and cardiac rehabilitation) and Neurodevelopmental Therapy section. Exclusions: Supportive care rendered primarily to maintain the level of correction already achieved; care rendered primarily for the convenience of the Enrollee; care rendered on a non-acute, asymptomatic basis; charges for any other services that do not meet KFHPWA clinical criteria as Medically Necessary Massage Therapy Massage therapy when in accordance with KFHPWA clinical After Deductible, Enrollee pays 15% Plan criteria, limited to a total of 24 visits per calendar year. Coinsurance for specialty care provider office visits PEBB_SCA_2024 29
 Kaiser Permanente WA SoundChoice EOC (2024) Page 28 Page 30
Kaiser Permanente WA SoundChoice EOC (2024) Page 28 Page 30