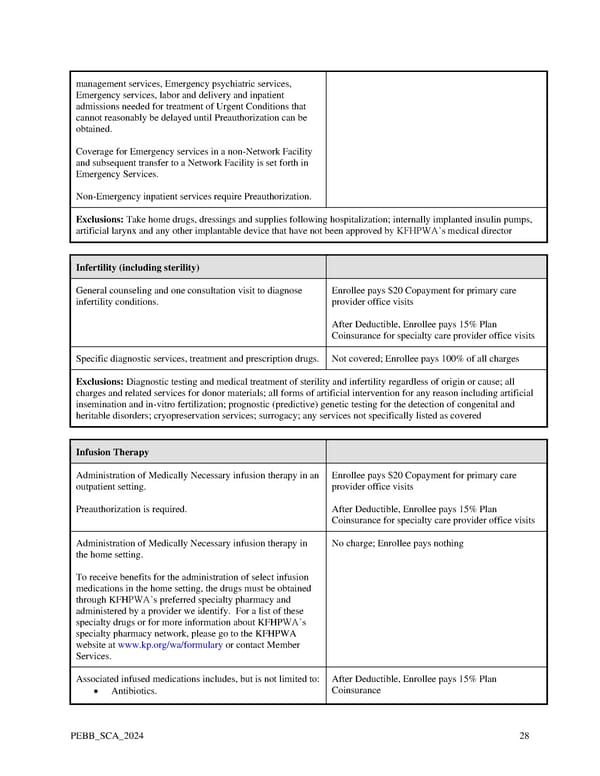
management services, Emergency psychiatric services, Emergency services, labor and delivery and inpatient admissions needed for treatment of Urgent Conditions that cannot reasonably be delayed until Preauthorization can be obtained. Coverage for Emergency services in a non-Network Facility and subsequent transfer to a Network Facility is set forth in Emergency Services. Non-Emergency inpatient services require Preauthorization. Exclusions: Take home drugs, dressings and supplies following hospitalization; internally implanted insulin pumps, artificial larynx and any other implantable device that have not been approved by KFHPWA’s medical director Infertility (including sterility) General counseling and one consultation visit to diagnose Enrollee pays $20 Copayment for primary care infertility conditions. provider office visits After Deductible, Enrollee pays 15% Plan Coinsurance for specialty care provider office visits Specific diagnostic services, treatment and prescription drugs. Not covered; Enrollee pays 100% of all charges Exclusions: Diagnostic testing and medical treatment of sterility and infertility regardless of origin or cause; all charges and related services for donor materials; all forms of artificial intervention for any reason including artificial insemination and in-vitro fertilization; prognostic (predictive) genetic testing for the detection of congenital and heritable disorders; cryopreservation services; surrogacy; any services not specifically listed as covered Infusion Therapy Administration of Medically Necessary infusion therapy in an Enrollee pays $20 Copayment for primary care outpatient setting. provider office visits Preauthorization is required. After Deductible, Enrollee pays 15% Plan Coinsurance for specialty care provider office visits Administration of Medically Necessary infusion therapy in No charge; Enrollee pays nothing the home setting. To receive benefits for the administration of select infusion medications in the home setting, the drugs must be obtained through KFHPWA’s preferred specialty pharmacy and administered by a provider we identify. For a list of these specialty drugs or for more information about KFHPWA’s specialty pharmacy network, please go to the KFHPWA website at www.kp.org/wa/formulary or contact Member Services. Associated infused medications includes, but is not limited to: After Deductible, Enrollee pays 15% Plan • Antibiotics. Coinsurance PEBB_SCA_2024 28
 Kaiser Permanente WA SoundChoice EOC (2024) Page 27 Page 29
Kaiser Permanente WA SoundChoice EOC (2024) Page 27 Page 29