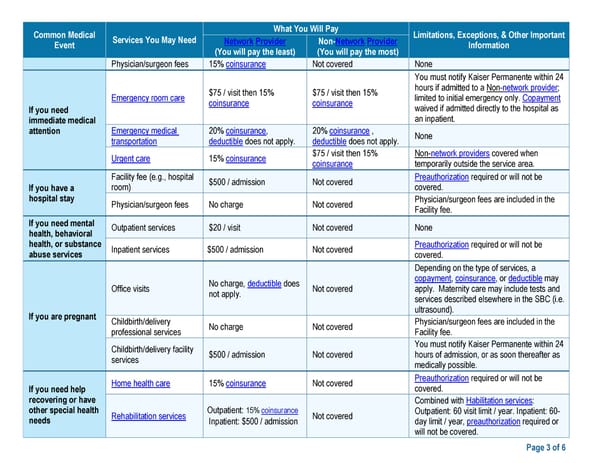
Common Medical What You Will Pay Limitations, Exceptions, & Other Important Event Services You May Need Network Provider Non-Network Provider Information (You will pay the least) (You will pay the most) Physician/surgeon fees 15% coinsurance Not covered None You must notify Kaiser Permanente within 24 $75 / visit then 15% $75 / visit then 15% hours if admitted to a Non-network provider; Emergency room care coinsurance coinsurance limited to initial emergency only. Copayment If you need waived if admitted directly to the hospital as immediate medical an inpatient. attention Emergency medical 20% coinsurance, 20% coinsurance , None transportation deductible does not apply. deductible does not apply. Urgent care 15% coinsurance $75 / visit then 15% Non-network providers covered when coinsurance temporarily outside the service area. Facility fee (e.g., hospital $500 / admission Not covered Preauthorization required or will not be If you have a room) covered. hospital stay Physician/surgeon fees No charge Not covered Physician/surgeon fees are included in the Facility fee. If you need mental Outpatient services $20 / visit Not covered None health, behavioral health, or substance Inpatient services $500 / admission Not covered Preauthorization required or will not be abuse services covered. Depending on the type of services, a No charge, deductible does copayment, coinsurance, or deductible may Office visits not apply. Not covered apply. Maternity care may include tests and services described elsewhere in the SBC (i.e. If you are pregnant ultrasound). Childbirth/delivery No charge Not covered Physician/surgeon fees are included in the professional services Facility fee. Childbirth/delivery facility You must notify Kaiser Permanente within 24 services $500 / admission Not covered hours of admission, or as soon thereafter as medically possible. Home health care 15% coinsurance Not covered Preauthorization required or will not be If you need help covered. recovering or have Combined with Habilitation services: other special health Rehabilitation services Outpatient: 15% coinsurance Not covered Outpatient: 60 visit limit / year. Inpatient: 60- needs Inpatient: $500 / admission day limit / year, preauthorization required or will not be covered. Page 3 of 6
 Kaiser Permanente WA SoundChoice SBC (2024) Page 2 Page 4
Kaiser Permanente WA SoundChoice SBC (2024) Page 2 Page 4