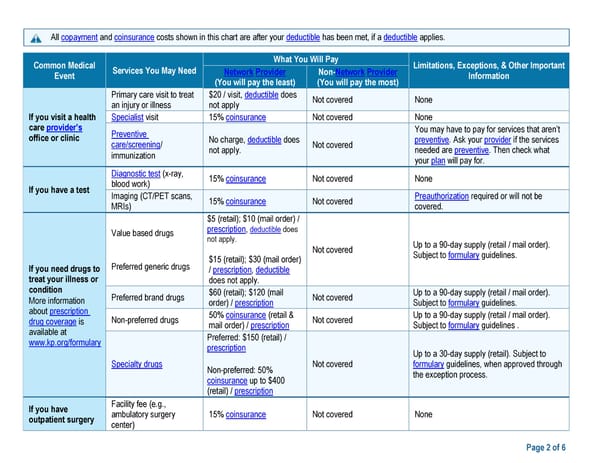
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies. Common Medical What You Will Pay Limitations, Exceptions, & Other Important Event Services You May Need Network Provider Non-Network Provider Information (You will pay the least) (You will pay the most) Primary care visit to treat $20 / visit, deductible does Not covered None an injury or illness not apply If you visit a health Specialist visit 15% coinsurance Not covered None care provider’s office or clinic Preventive You may have to pay for services that aren’t care/screening/ No charge, deductible does Not covered preventive. Ask your provider if the services immunization not apply. needed are preventive. Then check what your plan will pay for. Diagnostic test (x-ray, 15% coinsurance Not covered None If you have a test blood work) Imaging (CT/PET scans, 15% coinsurance Not covered Preauthorization required or will not be MRIs) covered. $5 (retail); $10 (mail order) / Value based drugs prescription, deductible does not apply. Up to a 90-day supply (retail / mail order). Not covered Subject to formulary guidelines. If you need drugs to Preferred generic drugs $15 (retail); $30 (mail order) treat your illness or / prescription, deductible condition does not apply. More information Preferred brand drugs $60 (retail); $120 (mail Not covered Up to a 90-day supply (retail / mail order). about prescription order) / prescription Subject to formulary guidelines. drug coverage is Non-preferred drugs 50% coinsurance (retail & Not covered Up to a 90-day supply (retail / mail order). available at mail order) / prescription Subject to formulary guidelines . www.kp.org/formulary Preferred: $150 (retail) / prescription Up to a 30-day supply (retail). Subject to Specialty drugs Not covered formulary guidelines, when approved through Non-preferred: 50% the exception process. coinsurance up to $400 (retail) / prescription If you have Facility fee (e.g., outpatient surgery ambulatory surgery 15% coinsurance Not covered None center) Page 2 of 6
 Kaiser Permanente WA SoundChoice SBC (2024) Page 1 Page 3
Kaiser Permanente WA SoundChoice SBC (2024) Page 1 Page 3