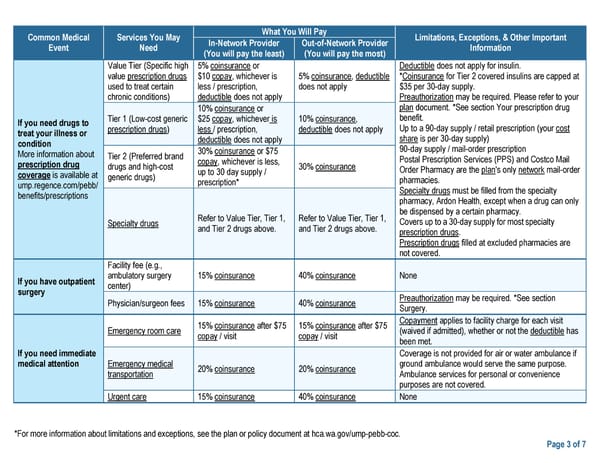
Common Medical Services You May What You Will Pay Limitations, Exceptions, & Other Important Event Need In-Network Provider Out-of-Network Provider Information (You will pay the least) (You will pay the most) Value Tier (Specific high 5% coinsurance or Deductible does not apply for insulin. value prescription drugs $10 copay, whichever is 5% coinsurance, deductible *Coinsurance for Tier 2 covered insulins are capped at used to treat certain less / prescription, does not apply $35 per 30-day supply. chronic conditions) deductible does not apply Preauthorization may be required. Please refer to your 10% coinsurance or plan document. *See section Your prescription drug If you need drugs to Tier 1 (Low-cost generic $25 copay, whichever is 10% coinsurance, benefit. treat your illness or prescription drugs) less / prescription, deductible does not apply Up to a 90-day supply / retail prescription (your cost condition deductible does not apply share is per 30-day supply) More information about Tier 2 (Preferred brand 30% coinsurance or $75 90-day supply / mail-order prescription prescription drug drugs and high-cost copay, whichever is less, 30% coinsurance Postal Prescription Services (PPS) and Costco Mail coverage is available at generic drugs) up to 30 day supply / Order Pharmacy are the plan's only network mail-order ump.regence.com/pebb/ prescription* pharmacies. benefits/prescriptions Specialty drugs must be filled from the specialty pharmacy, Ardon Health, except when a drug can only Refer to Value Tier, Tier 1, Refer to Value Tier, Tier 1, be dispensed by a certain pharmacy. Specialty drugs and Tier 2 drugs above. and Tier 2 drugs above. Covers up to a 30-day supply for most specialty prescription drugs. Prescription drugs filled at excluded pharmacies are not covered. Facility fee (e.g., If you have outpatient ambulatory surgery 15% coinsurance 40% coinsurance None surgery center) Physician/surgeon fees 15% coinsurance 40% coinsurance Preauthorization may be required. *See section Surgery. 15% coinsurance after $75 15% coinsurance after $75 Copayment applies to facility charge for each visit Emergency room care copay / visit copay / visit (waived if admitted), whether or not the deductible has been met. If you need immediate Coverage is not provided for air or water ambulance if medical attention Emergency medical 20% coinsurance 20% coinsurance ground ambulance would serve the same purpose. transportation Ambulance services for personal or convenience purposes are not covered. Urgent care 15% coinsurance 40% coinsurance None *For more information about limitations and exceptions, see the plan or policy document at hca.wa.gov/ump-pebb-coc. Page 3 of 7
 UMP Classic Medicare SBC (2024) Page 2 Page 4
UMP Classic Medicare SBC (2024) Page 2 Page 4