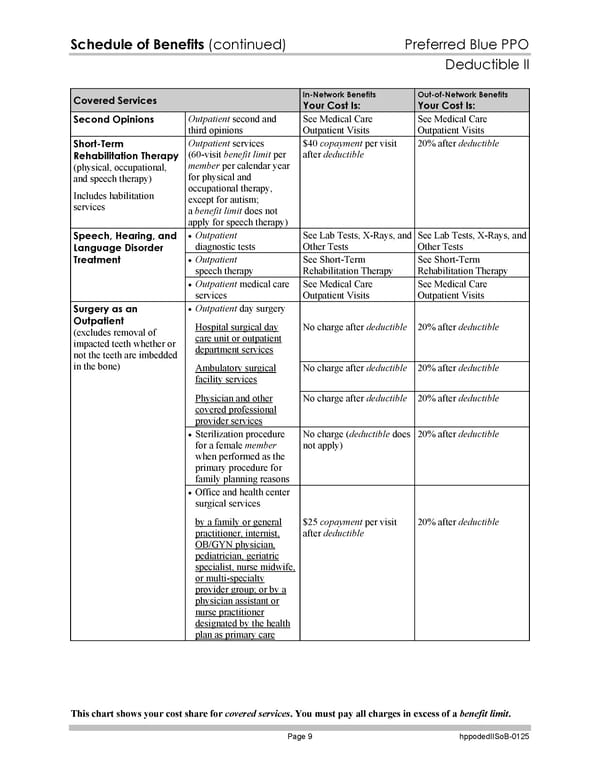
Schedule of Benefits (continued) Preferred Blue PPO Deductible II This chart shows your cost share for covered services. You must pay all charges in excess of a benefit limit. Page 9 hppodedIISoB-0125 Covered Services In-Network Benefits Your Cost Is: Out-of-Network Benefits Your Cost Is: Second Opinions Outpatient second and third opinions See Medical Care Outpatient Visits See Medical Care Outpatient Visits Short-Term Rehabilitation Therapy (physical, occupational, and speech therapy) Includes habilitation services Outpatient services (60-visit benefit limit per member per calendar year for physical and occupational therapy, except for autism; a benefit limit does not apply for speech therapy) $40 copayment per visit after deductible 20% after deductible Outpatient diagnostic tests See Lab Tests, X-Rays, and Other Tests See Lab Tests, X-Rays, and Other Tests Outpatient speech therapy See Short-Term Rehabilitation Therapy See Short-Term Rehabilitation Therapy Speech, Hearing, and Language Disorder Treatment Outpatient medical care services See Medical Care Outpatient Visits See Medical Care Outpatient Visits Outpatient day surgery Hospital surgical day care unit or outpatient department services No charge after deductible 20% after deductible Ambulatory surgical facility services No charge after deductible 20% after deductible Physician and other covered professional provider services No charge after deductible 20% after deductible Sterilization procedure for a female member when performed as the primary procedure for family planning reasons No charge (deductible does not apply) 20% after deductible Office and health center surgical services Surgery as an Outpatient (excludes removal of impacted teeth whether or not the teeth are imbedded in the bone) by a family or general practitioner, internist, OB/GYN physician, pediatrician, geriatric specialist, nurse midwife, or multi-specialty provider group; or by a physician assistant or nurse practitioner designated by the health plan as primary care $25 copayment per visit after deductible 20% after deductible
 Subscriber Certificate and Rider Documentation Page 135 Page 137
Subscriber Certificate and Rider Documentation Page 135 Page 137