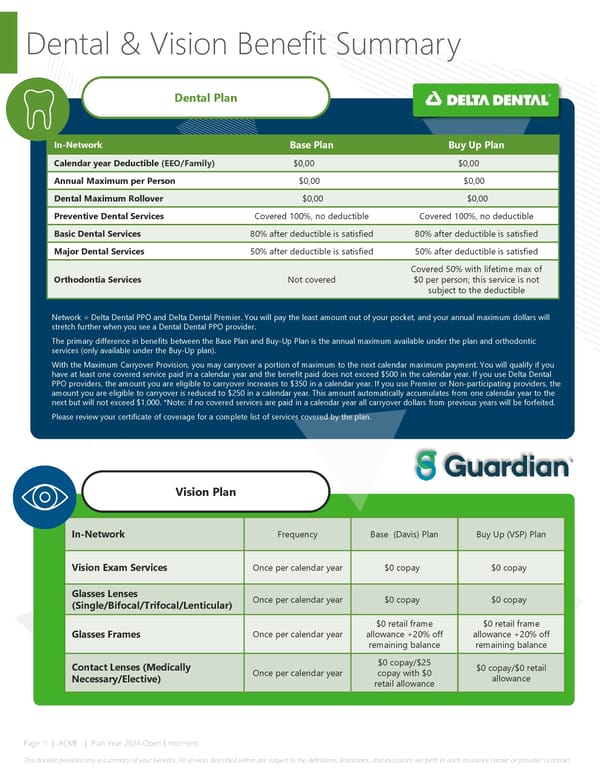
Dental & Vision Benefit Summary Dental Plan In-Network Base Plan Buy Up Plan Calendar year Deductible (EEO/Family) $0,00 $0,00 Annual Maximum per Person $0,00 $0,00 Dental Maximum Rollover $0,00 $0,00 Preventive Dental Services Covered 100%, no deductible Covered 100%, no deductible Basic Dental Services 80% after deductible is satisfied 80% after deductible is satisfied Major Dental Services 50% after deductible is satisfied 50% after deductible is satisfied Covered 50% with lifetime max of Orthodontia Services Not covered $0 per person; this service is not subject to the deductible Network = Delta Dental PPO and Delta Dental Premier. You will pay the least amount out of your pocket, and your annual maximum dollars will stretch further when you see a Dental Dental PPO provider. The primary difference in benefits between the Base Plan and Buy-Up Plan is the annual maximum available under the plan and orthodontic services (only available under the Buy-Up plan). With the Maximum Carryover Provision, you may carryover a portion of maximum to the next calendar maximum payment. You will qualify if you have at least one covered service paid in a calendar year and the benefit paid does not exceed $500 in the calendar year. If you use Delta Dental PPO providers, the amount you are eligible to carryover increases to $350 in a calendar year. If you use Premier or Non-participating providers, the amount you are eligible to carryover is reduced to $250 in a calendar year. This amount automatically accumulates from one calendar year to the next but will not exceed $1,000. *Note: if no covered services are paid in a calendar year all carryover dollars from previous years will be forfeited. Please review your certificate of coverage for a complete list of services covered by the plan. Vision Plan In-Network Frequency Base (Davis) Plan Buy Up (VSP) Plan Vision Exam Services Once per calendar year $0 copay $0 copay Glasses Lenses Once per calendar year $0 copay $0 copay (Single/Bifocal/Trifocal/Lenticular) $0 retail frame $0 retail frame Glasses Frames Once per calendar year allowance +20% off allowance +20% off remaining balance remaining balance Contact Lenses (Medically $0 copay/$25 $0 copay/$0 retail Necessary/Elective) Once per calendar year copay with $0 allowance retail allowance Page 11 | ACME | Plan Year 2024 Open Enrollment This booklet provides only a summary of your benefits. All services described within are subject to the definitions, limitations, and exclusions set forth in each insurance carrier or provider’s contract.
 2024 Cobra Benefits Guide Page 10 Page 12
2024 Cobra Benefits Guide Page 10 Page 12