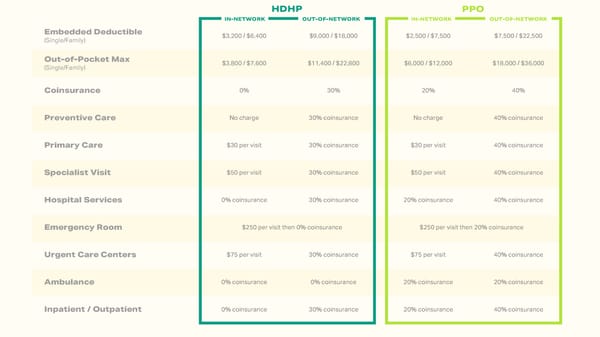
HDHP PPO IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK Embedded Deductible $3,200 / $6,400 $9,000 / $18,000 $2,500 / $7,500 $7,500 / $22,500 (Single/Family) Out-of-Pocket Max $3,800 / $7,600 $11,400 / $22,800 $6,000 / $12,000 $18,000 / $36,000 (Single/Family) Coinsurance 0% 30% 20% 40% Preventive Care No charge 30% coinsurance No charge 40% coinsurance Primary Care $30 per visit 30% coinsurance $30 per visit 40% coinsurance Specialist Visit $50 per visit 30% coinsurance $50 per visit 40% coinsurance Hospital Services 0% coinsurance 30% coinsurance 20% coinsurance 40% coinsurance Emergency Room $250 per visit then 0% coinsurance $250 per visit then 20% coinsurance Urgent Care Centers $75 per visit 30% coinsurance $75 per visit 40% coinsurance Ambulance 0% coinsurance 0% coinsurance 20% coinsurance 20% coinsurance Inpatient / Outpatient 0% coinsurance 30% coinsurance 20% coinsurance 40% coinsurance
 LHD Benefit Advisors 2024 Employee Benefits Page 5 Page 7
LHD Benefit Advisors 2024 Employee Benefits Page 5 Page 7