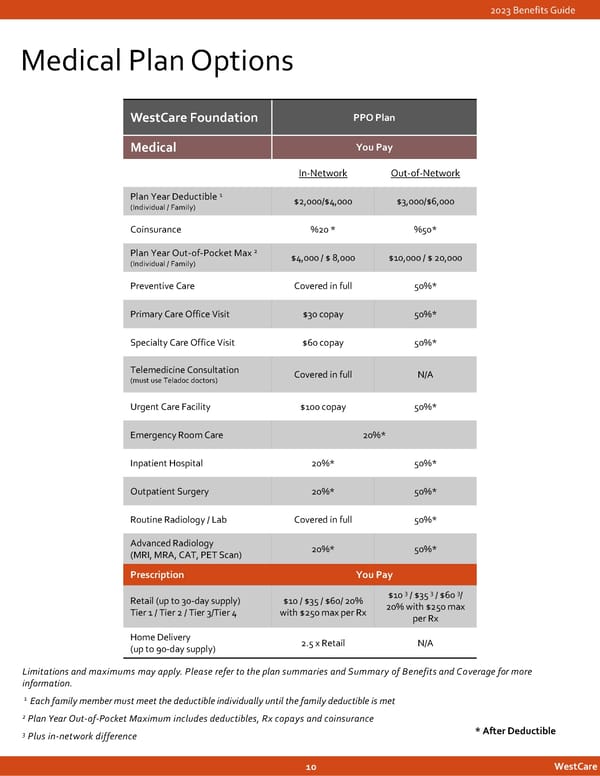
2023 Benefits Guide Medical Plan Options WestCareFoundation PPO Plan Medical You Pay In-Network Out-of-Network Plan Year Deductible 1 $2,000/$4,000 $3,000/$6,000 (Individual / Family) Coinsurance %20 * %50* Plan Year Out-of-Pocket Max 2 $4,000 / $ 8,000 $10,000 / $ 20,000 (Individual / Family) Preventive Care Covered in full 50%* Primary Care Office Visit $30 copay 50%* Specialty Care Office Visit $60 copay 50%* Telemedicine Consultation Covered in full N/A (must use Teladoc doctors) Urgent Care Facility $100 copay 50%* Emergency Room Care 20%* Inpatient Hospital 20%* 50%* Outpatient Surgery 20%* 50%* Routine Radiology / Lab Covered in full 50%* Advanced Radiology 20%* 50%* (MRI, MRA, CAT, PET Scan) Prescription You Pay 3 3 3 Retail (up to 30-day supply) $10 / $35 / $60/ 20% $10 / $35 / $60 / Tier 1 / Tier 2 / Tier 3/Tier 4 with $250 max per Rx 20% with $250 max per Rx Home Delivery 2.5 x Retail N/A (up to 90-day supply) Limitations and maximums may apply. Please refertothe plan summaries and Summary of Benefits and Coverage formore information. 1 Each family member must meet the deductible individually until the family deductible is met 2 Plan Year Out-of-Pocket Maximum includes deductibles, Rx copays and coinsurance 3 Plus in-network difference *After Deductible 10 WestCare
 2023 | Employee Benefits Guide Page 9 Page 11
2023 | Employee Benefits Guide Page 9 Page 11